


ABSTRACT
KEYWORDS
INTRODUCTION
MATERIALS AND METHODS
This study was conducted in a tertiary healthcare centre between January 1, 2008 and June 30, 2023. All paediatric patients aged between 0-18 years old who underwent appendectomy with a preliminary diagnosis of AA were quarried through the hospital record system retrospectively. The patients’ histopathological reports were reviewed for E. vermicularis. The study group consisted of the patients having appendectomy specimens containing the parasite whereas the members of the control group had AA without enterobiasis and operated during the same period. Two groups were matched according to age randomly. The information about socio-demographic and clinical features at the time of operation (age, sex, place of residence, number of siblings, number of household members, water supply, private room for children in the house, maternal and paternal education levels; existence of the pruritus ani, abdominal pain, nausea, vomiting, difficulty in defecation, fever at the time of hospital admission) were obtained by the structured questionnaire prepared by the researchers and filled on phone calls. The patients whose questionnaires were not fully filled were excluded. The total number of pediatric appendectomies performed during the study period based on clinical and radiologic diagnosis of AA was 3300, and the rate of enterobiasis was 1.6% (n= 53). After exclusion, 46 patients with EAAA and a control group matched according to age with NEAAA were determined. The data of 92 cases were evaluated. Body mass indexes were calculated through hospital records and grouped according to the growth charts based on age and sex for Turkish children (Thin: < 5%; Average: 5-95%; Obese: >95%) (21). Laboratory data [initial complete blood count (CBC), C-reactive protein (CRP), serum sodium, blood urea nitrogen/ creatinine ratio (BUN/Cr)], urine density, and radiologic reports were documented and recorded through hospital’s electronic data system. White blood cells (WBC), neutrophils and CRP were defined as “acute phase reactants” and analysed to identify systemic inflammatory response. Serum sodium, BUN/Cr and urine density were taken into consideration as the premonitory markers of dehydration. Serum bilirubin level was evaluated to be a follow up marker of complicated appendicitis (4,22).Ultrasonography diagnosis of AA was confirmed when the appendix was enlarged (appendiceal diameter measured ≥6 mm) and/or noncompressible.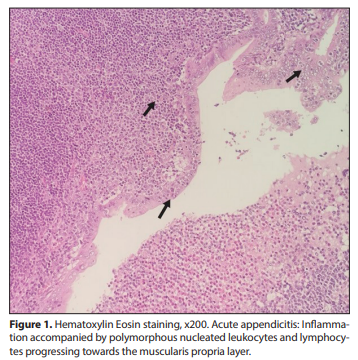
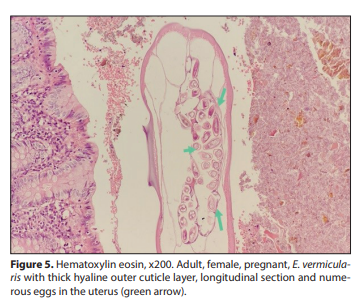
All appendectomy materials were examined histologically in our hospital within a routine procedure: The specimens were fixated in 10% formalin for 24 hours and four samples of five microns thickness were dissected for evaluation. After macroscopic evaluation, Hematoxylin-eosin stained slides were examined under a microscope. Clinical diagnoses and microscopic examination results were recorded. The cases in which neutrophil infiltration was observed in the muscularis propria of the appendix were defined as “AA” histopathologically (Figure 1). The specimens of the two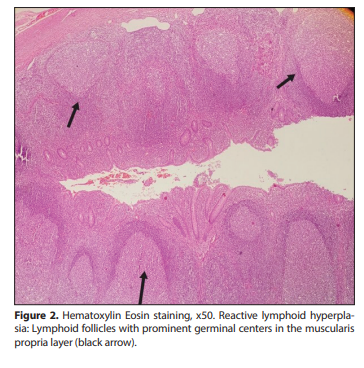
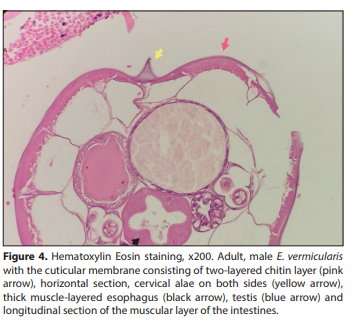
groups were re-evaluated and reported as LH (Figure 2), congestion, periappendicitis, hemorrhagic appendicitis, perforated appendicitis, abscess, phlegmonous appendicitis, gangrenous appendicitis, necrotizing appendicitis and E. vermicularis with or without peritonitis (Figure 3). The samples having hemorrhage, perforation, abscess, necrotizing, phlegmanous and/or gangrenous features were defined to be “complicated appendicitis.” E. vermicularis cases underwent additional procedures: Histochemical staining was performed with Periodic acid- Schiff (PAS) dye to evaluate the cuticular membrane consisting of a two-layered chitin layer, thick musclelayered esophagus, cervical alae, intestinal walls, uterus and testicular tissue of the nematode, which were pathognomonic in histopathological diagnosis of enterobiasis (Figure 4, 5).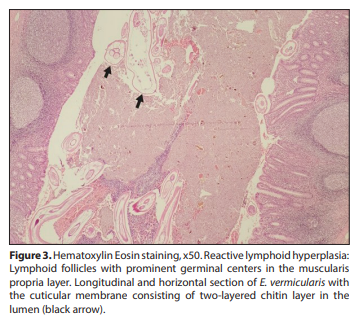
Statistical Analysis The analyses were performed by statistical package program software. The data were presented as percentages, frequencies, medians and minimum-maximum ranges or mean and standard deviation (SD) by descriptive statistics. Independent samples t-test was applied for the analyses of normally distributed continuous variables; whereas Mann-Whitney U or Kruskal Wallis tests were applied for the evaluation of abnormally distributed variables with Bonferroni correction when indicated. Cross-tables with chi-square test (χ2) and Fisher’s exact test were performed for the evaluation of categorical variables. Probability factor (p) less than 0.05 was regarded to be statistically significant. The study was approved by the Ethics Committee of NonInvasive Clinical Research of Amasya University (registration no: E-76988455-050.01.04-135458).
RESULTS
DISCUSSION
E. vermicularis is a nematode requiring a human host and completing its life cycle usually in the different parts of the gastrointestinal tract. During its migration, when it visits the appendix, it may cause “appendiceal colic” and the story ends with appendectomy.
| Study Group (Enterobiasis) | Control Group (Non-enterobiasis) | p | |
|---|---|---|---|
| Sex |
Male/Female (n= 21; 45.70 / n= 25; 54.3%) |
Male/Female (n= 19; 41.3% / n= 27; 58.7%) |
0.84 |
| Number of siblings | 2 (1-5) | 2 (1-4) | 0.55 |
|
Residence
Urban area
Rural area |
19.6% (n= 9) 71.7% (n= 33) |
67.4% (n= 31) 32.6% (n= 15) |
<0.0001 |
|
Income level
Low
Intermediate High |
26% (n= 12) 58.7% (n= 27) 4.3% (n= 2) |
17.4% (n= 8) 50.0% (n= 23) 32.6% (n= 15) |
0.001 |
|
Household members
<6
≥6 |
19.6% (n= 9) 80.4% (n= 37) |
26.1% (n= 12) 73.9% (n= 34) |
0.310 |
|
Water supply
Mains water
Spring water |
65.2% (n= 30) 34.8% (n= 16) |
84.8% (n= 39) 15.2% (n= 7) |
0.026 |
|
A private room for children
Yes
No |
36.1% (n= 22) 63.9% (n= 24) |
84.8% (n= 39) 15.2% (n= 7) |
<0.0001 |
|
Maternal education
Primary education
Secondary education High education |
45.7% (n= 21) 43.5% (n= 20) 10.9% (n= 5) |
13% (n= 6) 41.3% (n= 19) 45.7% (n= 21) |
<0.0001 |
|
Paternal education
Primary education
Secondary education Higher education |
50.0% (n= 23) 37.0% (n= 17) 13.0% (n= 6) |
13% (n= 6) 39.1% (n= 18) 47.8% (n= 22) |
<0.0001 |
|
Body mass index
<5%
5-95% >95% |
39.1% (n= 18) 52.2% (n= 24) 8.7% (n= 4) |
10.9% (n= 5) 52.2% (n= 24) 37% (n= 17) |
<0.0001 |
|
Pruritus ani
Yes
No |
78.3% (n= 36) 21.7% (n= 10) |
10.9% (n= 5) 89.1% (n= 41) |
<0.0001 |
|
Abdominal pain
Yes
No |
80.4% (n= 37) 19.6% (n= 9) |
84.8% (n= 39) 15.2% (n= 7) |
0.39 |
|
Nausea
Yes
No |
82.6% (n= 38) 17.4% (n= 8) |
87.0% (n= 40) 13.0% (n= 6) |
0.38 |
|
Vomiting
Yes
No |
21.7% (n= 10) 78.3% (n= 36) |
80.4% (n= 37) 19.6% (n= 9) |
<0.0001 |
|
Difficulty in defecation
Yes
No |
21.7% (n= 10) 78.3% (n= 36) |
89.1% (n= 41) 10.9% (n= 5) |
<0.0001 |
|
Fever (≥38 °C)
Yes
No |
17.4% (n= 8) 77.6% (n= 38) |
76.1% (n= 35) 22.4% (n= 11) |
<0.0001 |
| WBC (/mm³) (mean ± SD) | 11240 ± 4030 | 14530 ± 5900 | 0.002 |
| Neutrophils (min-max) | 8590 (1790-17840) | 10500 (1500-29300) | 0.005 |
| Lymphocytes (/mm³) | 2100 ± 980 | 2200 ± 1110 | 0.655 |
| Eosinophils (/mm³) | 100 (0-800) | 50 (0-410) | 0.004 |
| Neutrophils (%) | 71.3 (4.67-94.5) | 78.1 (32.8-92.3) | 0.256 |
| Lymphocytes (%) | 20 (5-50) | 13.1 (4-55.5) | 0.064 |
| Eosinophils (%) | 1 (0-9.2) | 0.15 (0-3.6) | <0.0001 |
| CRP (mg/dL) | 1.67 (0.5-89.9) | 12.5 (0.25-172.8) | <0.0001 |
| Bilirubin (mg/dL) | 0.38 (0.1-2.1) | 0.15 (0.15-1.6) | 0.30 |
| BUN/Creatinine | 40.24 ± 20.91 | 48.04 ± 17.69 | 0.06 |
| Sodium (mEq/mL) | 137 (121-144) | 137 (131-145) | 0.584 |
| Urine density | 1020 (1010-1030) | 1018 (1001-1065) | 0.819 |
| Ultrasonographic appendix diameter | 6.5 ± 1.12 | 9.05 ± 2.60 | 0.002 |
|
Ultrasonographic diagnosis
AA
Normal |
19.6%; n= 9 10.9%; n= 5 |
32.6%; n= 15 2.2%; n= 1 |
0.001 <0.0001 |
|
Histopathological evaluation
AA
Complicated appendicitis Reactive lymphoid hyperplasia |
37.9%; n= 17 4.3%; n= 2 58.7%; n= 27 |
26.1%; n= 12 73.9%; n= 34 0%; n= 0 |
<0.0001 |