ABSTRACT
KEYWORDS
INTRODUCTION
MATERIALS AND METHODS
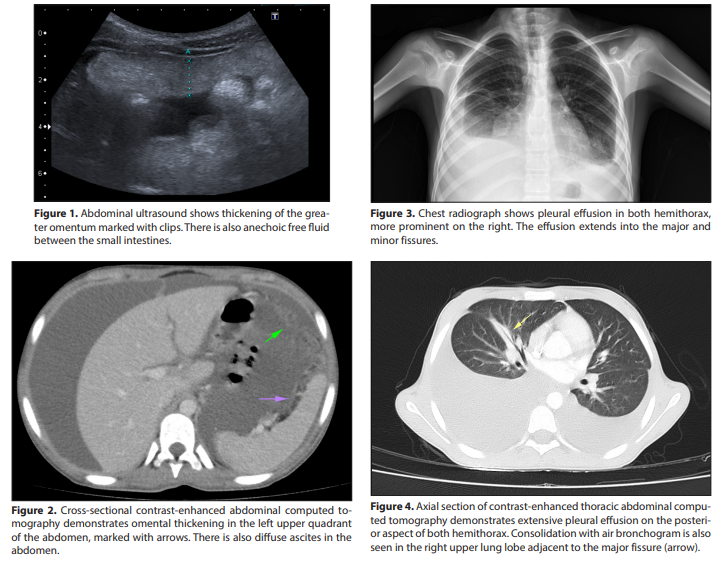
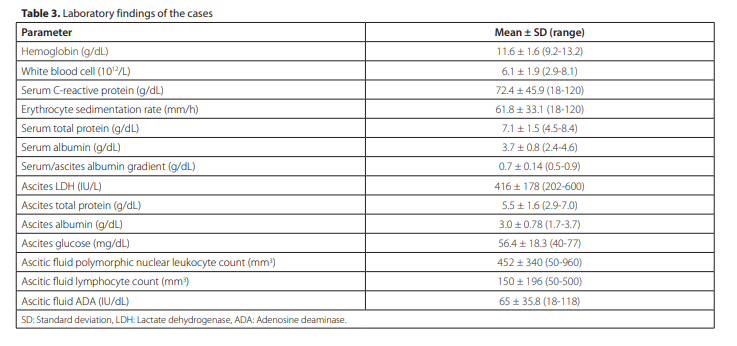
Five cases diagnosed with TB peritonitis were examined. Three of the cases were female and two were male, and median age was 12 years (range: 7.5 to 16 years). All cases presented with complaints of abdominal distension. In addition, three cases had complaints of abdominal pain and weight loss. One case had respiratory distress. Two of the cases had cough, night sweats, and fever. Median duration of symptoms was 57 days (range: 15 to 90 days). Median time to diagnosis was 14 days (range: 12 to 15 days). None of the cases had a history of contact with TB. Demographic data and clinical findings of the cases are summarized in Table 1. All cases had TST, but only two of the patients had a Bacillus Calmette-Guérin vaccination scar at the time of presentation. Induration >15 mm was observed in only one case; this case was using adalimumab (third generation tumor necrosis factor inhibitor) for uveitis due to juvenile rheumatoid arthritis. Abdominal ultrasonography revealed diffuse ascites in the abdomen in all cases (Figure 1). Abdominal computed tomography revealed heterogeneity, thickening and diffuse ascites in the omentum in all cases (Figure 2). Bilateral extensive pleural effusion due to lung involvement was detected in one case (Figure 3). Thoracic computed tomography of the patient revealed extensive pleural effusion in both hemithorax and air bronchogram adjacent to the major fissure in the upper lobe of the right lung (Figure 4). Bilateral chest tube was inserted to drain the pleural effusion in this case. Radiological findings of the cases are presented in Table 2. Paracentesis was performed in all cases. In all cases, ascitic fluid was observed to be yellow and cloudy (exudate). Serumascitic albumin gradient (SAAG) was detected as <1.1 gr/dL. Complete blood count, blood biochemistry and ascitic fluid laboratory findings of the cases are shown in Table 3. Median adenosine deaminase (ADA) level of ascitic fluids was 65 U/L (range: 18 to 118 U/L). Microscopic examination of ascitic fluids
| Case No | 1 | 2 | 3 | 4 | 5 |
|---|---|---|---|---|---|
| Age (years) | 12 | 12 | 7.5 | 16 | 12 |
| Sex | Girl | Girl | Boy | Boy | Girl |
| Duration of complaints (days) | 60 | 30 | 15 | 90 | 60 |
| Complaints | |||||
| Abdominal distension | |||||
| Weight loss | Yes | Yes | No | No | Yes |
| Abdominal pain | Yes | Yes | No | No | Yes |
| Cough | Yes | Yes | No | No | No |
| Night sweats | Yes | Yes | No | No | No |
| Respiratory distress | Yes | No | No | No | No |
| Fever | Yes | Yes | No | No | No |
| BCG scar | Yes | No | No | No | Yes |
| Tuberculin PPD test results | Negative | Positive (15 mm) | Negative | Negative | Negative |
| Time of diagnosis (days) | 15th | 12nd | 13rd | 15th | 15th |
| Case No | 1 | 2 | 3 | 4 | 5 |
|---|---|---|---|---|---|
| Chest radiograph | Normal | Pleural effusion in both hemithoraxes, prominent on the right | Normal | Normal | Normal |
| Abdominal ultrasonography | Diffuse free fluid in the peritoneal cavity | Diffuse free fluid in the peritoneal cavity | Diffuse free fluid in the peritoneal cavity | Diffuse free fluid in the peritoneal cavity | Diffuse free fluid in the peritoneal cavity and thickening of the greater omentum |
| Contrast-enhanced abdominal tomography | Thickening of the omentum and diffuse free fluid in the peritoneal cavity | Thickening of the omentum and diffuse free fluid in the peritoneal cavity | Thickening of the omentum and diffuse free fluid in the peritoneal cavity | Thickening of the omentum and diffuse free fluid in the peritoneal cavity | Thickening of the omentum and diffuse free fluid in the peritoneal cavity |
| Thoracic tomography | Cavitary lesion in the lungs | Extensive pleural effusion in both hemithoraxes and air bronchogram adjacent to the major fissure in the upper lobe of the right lung | Normal | Normal | Normal |
| Laparoscopic findings | Inflammation in the peritoneum and serosal membranes | Diffuse increased fragility of the peritoneum; adhesions and granulomatous thickening between intestinal loops and peritoneum | Diffuse increased fragility of the peritoneum; adhesions and granulomatous thickening between intestinal loops and peritoneum | Granulomatous thickening of the intestinal loops and omentum | Diffuse increased fragility and granulomatous thickening of the peritoneum |
| Peritoneal pathological examination | Non-necrotizing granulomatous peritonitis and sparsely located bacilli in AFB stain | Non-necrotizing granulomatous peritonitis | Non-necrotizing granulomatous peritonitis | Non-necrotizing granulomatous peritonitis | Non-necrotizing granulomatous peritonitis |
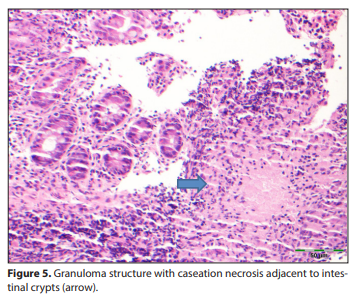
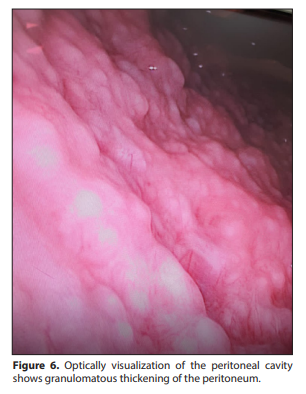
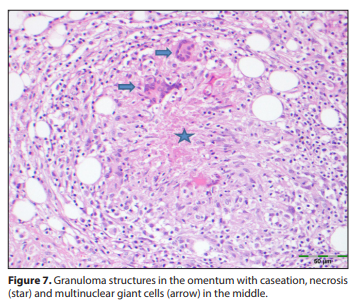
revealed abundant lymphocytes in three cases and abundant polymorphnuclear leukocytes in two cases. TB bacilli grew in the ascitic fluid and sputum cultures of one case. In this case, sparsely located bacilli in acid-fast bacilli (AFB) stain were seen in the peritoneal biopsy. TB bacilli polymerase chain reaction (PCR) was negative in ascitic fluid in all cases. A patient receiving adalimumab for uveitis due to juvenile rheumatoid arthritis had abdominal pain and diarrhea. This patient underwent colonoscopy after bowel preparation. Colonoscopy showed an edematous and hyperemic ileocecal valve. The terminal ileum could not be entered because of the risk of perforation. Histopathological examination of colon biopsies showed necrotizing granulomatous inflammation (intestinal TB) (Figure 5). Colonoscopy performed on this patient after treatment for TB showed complete resolution of the old lesions. All patients underwent diagnostic laparoscopy. During laparoscopic examination, it was observed that there was free fluid in the abdomen and the peritoneum was thick and fragile. Visualization with optically inserted trocar revealed adhesions and granulomatous thickening between the intestinal rings and the peritoneum in the abdomen that did not allow imaging (Figure 6). Histopathological examination of peritoneal biopsies revealed non-necrotizing granulomatous peritonitis (Figure 7). All cases received quadruple anti-TB treatment for 12 months. Urticarial reactions were observed in two cases due to isoniazid. In these two cases, isoniazid was stopped for a certain period and then restarted. One case with lung involvement was given corticosteroid treatment for four weeks. The cases were observed to recover completely with treatment. No problems were observed in the one-year follow-up after completion of treatment.