


ABSTRACT
KEYWORDS
INTRODUCTION
MATERIALS AND METHODS
RESULTS
Of the 22 cases included in the study, 13 (59.1%) were male and 9 (40.9%) were female. Eleven (50%) of our cases were aged 1-4 years, and 8 (36.3%) were aged 5-9 years. Twenty-one (95.4%) of our patients were Syrian refugees and had contact with measles patients in the surrounding area. One (4.5%) patient was fully vaccinated, had no history of contact, and had received all vaccinations, including measles, according to the Turkish Ministry of Health’s Childhood Vaccination Schedule. Two (9.5%) of the cases were younger than 12 months and had not received the measles vaccine, while 19 (90.4%) were older than 12 months but had not received any age-appropriate vaccines, including the measles vaccine (Table 1). The symptoms and findings at the time of presentation were: high fever (100%), maculopapular rash (95.5%), sore throat (59.1%), Koplik spots (59.1%), runny nose (54.5%), fatigue/lethargy (50%), conjunctivitis (36.4%), decreased oral intake (28.6%), cough (27.3%), dehydration (18.2%),tachypnea (9.1%), rales/rhonchi on lung auscultation (9.1%),diarrhea (4.5%), and lymphadenitis (4.5%). The most common presenting complaints were high fever and rash (Table 2).
| Variables | n (%) |
|---|---|
|
Total number of patients
Female
Male |
22
9 (40.9)
13 (59.1) |
|
Age distribution of the patients
<12 month
1-4 y 5-9 y 10-15 y |
2 (9.1) 11 (50) 8 (36.3) 1 (4.6) |
|
Vaccination status
<9 month (unvaccinated)
>9 month (vaccinated) >9 month (unvaccinated) |
1 (4.5) 1 (4.5) 20 (90.9) |
| Signs | Number of Patients n (%) |
|---|---|
| Fever | 22 (100%) |
| Runny nose/Cold | 12 (54.5%) |
| Sore throat | 13 (59.1%) |
| Cough | 6 (27.3%) |
| Fatigue/Weakness | 11 (50%) |
| Watery eyes | 8 (36.4%) |
| Diarrhea | 1 (4.5%) |
| Poor oral intake | 6 (28.6%) |
| Symptoms | |
| Maculopapular rash | 21 (95.5%) |
| Koplik spots | 13 (59.1%) |
| Conjunctivitis | 8 (36.4%) |
| Lymphadenopathy | 1 (4.5%) |
| Tachypnea | 2 (9.1%) |
| Rales/Rhonchi on auscultation | 2 (9.1%) |
| Oxygen requirement | 2 (9.1%) |
| Dehydration | 4 (18.2%) |
| Hemogram | Median | Average Value | Minimum-Maximum Value |
|---|---|---|---|
| Leukocyte (mm³) | 7260 ± 3350 | 4000-18330 | |
| Neutrophil (mm³) | 3110 ± 1960 | 2130-9650 | |
| Lymphocyte (mm³) | 3410 ± 2260 | 720-9650 | |
| Hemoglobin (g/dL) | 11.7 ± 2.4 | 6.6-16.6 | |
| Platelet (mm³) | 280000 ± 64559 | 177000-409000 | |
| Biochemical values | |||
| ALT (U/L) | 16 | 9-124 | |
| AST (U/L) | 40 ± 18 | 20-95 | |
| LDH (U/L) | 420 ± 79 | 259-572 | |
| Creatinine (mg/dL) | 0.4 ± 0.16 | 0.16-0.83 | |
| CRP (mg/dL) | 8.4 | 3-130 | |
DISCUSSION
The age range in our study group was 7-167 months, with a median age of 44 months. In a study conducted in Ankara in 2012 with 44 measles cases, the age range was 4-191 months, with an average age of 58.6 ± 59.5 months (8). In the 2013-2014 epidemic in Istanbul, the age range was 7-196 months and the mean age was 63.8 ± 44 months in 20 cases (9). Yıldırım et al. reported that the median age of 131 patients in the 2012- 2014 epidemic in İstanbul was 50.5 (2-216) months (10). In 2019, Demir et al. studied 20 measles cases in Diyarbakır, with an age range of 5-214 months and a median age of 11 months (range 8-27) (11). In the study by Tepebaşılı et al., the median value was 5-156 months (12). When the age distribution of the patients in our study was compared with other studies, our study was similar to the study by Tepebaşılı et al. (12). In our study group, there were 13 (59.1%) male and 9 (40.9%) female patients. The male/female ratio was 1.4/1. When we compared male and female patients in our study, we found a significant difference between the sexes (p= 0.049). Metin et al. have reported a male/female ratio of 1.7/1 in 44 measles cases in their study from Ankara, and Türkkan et al. have reported a male/female ratio of 1.5/1 in their study of 20 measles patients from İstanbul (8-9). These ratios were similar to those found in our study. However, it should be kept in mind that in the absence of measles immunization, everyone is susceptible to the disease at any age, regardless of sex. In communities with insufficient measles vaccination coverage, outbreaks are inevitable in the presence of susceptible individuals. In Türkiye, the vaccination rate among children aged 9 months to 6 years was increased to 96.3% in 2005, in line with the WHO’s “Measles Elimination in Europe by 2010” plan (13). The number of measles cases in our country was 7,820 in 2002, but after the vaccination campaign, it decreased to zero cases in 2009 (14). After 2011, a measles outbreak was reported, in which the vast majority of cases occurred in Istanbul and it was thought to originate from imported cases (15). Twenty-one (95.4%) of our cases were Syrian refugees, all of whom were unvaccinated. The number of cases who had contact with a measles patient was 20 (90.9%). Tepebaşılı et al. reported the proportion of unvaccinated patients as 84.7%, while Türkkan et al. reported it as 85% (9,12). In our study, the proportion of unvaccinated patients was 95.2%. In a meta-analysis of cohort studies, the effectiveness of one dose of a measles-containing vaccine in children is 95% [95% confidence interval (CI), 87-98%] after one dose and 96% (95% CI, 71-99%) after two doses (16). Measles outbreaks are mostly seen in unvaccinated individuals. When measles occurs in individuals who have received ≥2 doses of the measles-containing vaccine, it is less severe than in those who have received only one dose or who are unvaccinated (17). Among our cases, we identified the disease in a 14-year-old male patient who had been vaccinated with two doses of the measles vaccine. High fever was the most prominent symptom in all of our cases. This was similar to other studies (8-11). Maculopapular rash was observed in 21 (95.5%) of our patients. The rash started on the face and scalp and spread to the trunk and extremities. Koplik spots were observed in 13 (59.1%) of our cases. However, the incidence of Koplik spots was found to be low in the studies conducted by Demir and Yıldırım and colleagues (10,11). Leukopenia, thrombocytopenia, and T-cell lymphopenia may be observed during measles infection (18,19). In our study, median leukocyte count was 7260 ± 3352/mm3 . Lymphopenia was present in 3 (13.6%) of our cases. No leukopenia or thrombocytopenia was detected in any of our patients. In other studies, leukopenia was detected in 11.2- 73% of the cases, and thrombocytopenia in 33.6-50% of the cases (20,21). Measles-specific IgM antibody begins to rise on the 1st and 2nd days of the rash and can remain in the serum until the 30th to 60th day (22). Similar to our study, Türkkan et al., Metin et al., and Yıldırım et al. have found a 100% positivity rate for measles-specific IgM in their studies of measles patients (8- 10). The most common complications of measles in children are otitis media, bronchopneumonia, croup, and diarrhea, with acute encephalitis causing permanent brain damage occurring at a rate of 0.1%. Deaths can occur at a rate of 0.1- 0.3% as a result of respiratory and neurological complications (17). In our study, we observed poor oral intake in five of the hospitalized cases, pneumonia in two, and diarrhea in one. Two of our hospitalized patients were admitted and treated for bronchopneumonia, and three for malnutrition. All our patients were discharged after recovery. Consistent with the literature, pneumonia constituted the majority of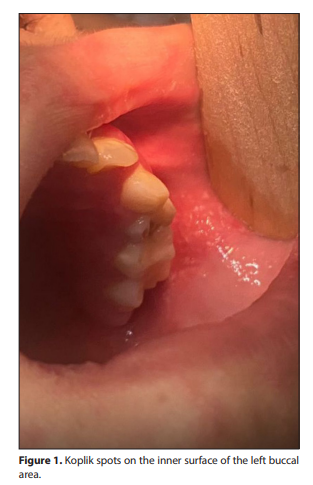
complications (20). Otitis, tracheitis, keratitis, encephalitis, Guillain-Barré syndrome, or death were not observed (23). Since there was no long-term follow-up of the cases, we do not have follow-up data on subacute sclerosing panencephalitis, which is one of the limitations of our study. Considering that the attack rate of the disease is 90%, the importance of early suspicion, early isolation, strict adherence to isolation measures, and contact prophylaxis is clearly evident. Especially in endemic areas, during outbreaks, when individuals, who are younger than 12 months and unvaccinated and who are known to be susceptible, present with respiratory symptoms, fever, and maculopapular rash, questioning and follow-up should be performed thoroughly, and in case of suspicion, the patient should be isolated. We hospitalized and followed up five of our patients. We did not see any measles cases among contacts associated with hospital admission. Furthermore, the presence of Koplik spots in the first migrant patient who presented to the emergency department with fever and rash was very helpful in diagnosing measles and monitoring contacts. With close monitoring of contacts, the outbreak in our province subsided in about three weeks. Figures 1 and 2 show the maculopapular rash and Koplik spots on the face.