


ABSTRACT
KEYWORDS
INTRODUCTION
The measles virus is an enveloped RNA virus belonging to the Paramyxoviridae family, with a single serotype, and causes disease only in humans. The absence of a natural animal reservoir and the existence of a single serotype make measles a biologically eradicable disease (1). However, the measles virus is divided into different genotypic subgroups that show genetic diversity at the molecular level. Genotypic classification based on the genetic diversity of the measles virus is used in molecular surveillance, outbreak investigations, and verification of measles elimination. However, it should be emphasized that despite this genetic variability, the measles virus has a single serotype and all circulating genotypes are preventable with currently available vaccines. Genotyping is performed based on sequence analysis of the 450-nucleotide region at the carboxyl terminus of the nucleoprotein gene (N-450), as recommended by the World Health Organization (WHO); this region is accepted as the international standard for classifying virus strains as genotypes (2). Historically, measles viruses have been classified into 8 clades (A-H), and a total of 24 genotypes have been identified; however, a significant portion of these genotypes are no longer considered active as they have not been detected for a long time (3). In recent years, global surveillance data has shown a marked decrease in the number of genotypes in circulation, with the B3 and D8 genotypes reported to be predominant in current outbreaks. This decline reflects the success of comprehensive immunization programs and molecular surveillance, while also highlighting the importance of the sustainability of virological surveillance in confirming measles elimination (4). Despite being a preventable disease with biologically feasible elimination thanks to effective and safe vaccines, measles continues to cause significant morbidity and mortality worldwide. Inadequate global vaccination rates, vaccine hesitancy, particularly in developed countries and in our country, migration, and international travel are causing the reemergence of measles and outbreaks even in areas where elimination had previously been achieved (1,5). Recently, it has been reported that eight countries, including the United States and Canada in North America and the United Kingdom in Europe, have lost their measles elimination status as of 2026 (6). This situation demonstrates that measles remains not only an individual clinical problem but also a significant public health threat (1,5). Post-exposure prophylaxis (PEP) for measles is a critical public health intervention aimed at preventing disease development after exposure or reducing disease severity, requiring timing according to the incubation period and appropriate patient selection (7). PEP, administered through vaccination or immunoglobulin (IG), plays a crucial role in preventing disease development and controlling outbreaks, particularly in individuals who are unvaccinated or immunocompromised (8). Measles, Rubella, and Congenital Rubella Syndrome Surveillance Field Guide of the Turkish Ministry of Health (2010), prepared in line with Türkiye’s measles elimination goals, is still in effect. However, it reflects the epidemiological conditions of the period in which it was published and does not comprehensively cover PEP approaches based on current national data and international guidelines (9). The limited information on PEP in the current guide may lead to differences in practices and increase the need for standardization in the field. The recommendations of the Pediatric Infectious Diseases and Immunization Society are to address PEP approaches in individuals exposed to measles in line with current scientific evidence, international guidelines, and existing legislation in Türkiye; and to provide a standard, applicable, and traceable approach for healthcare professionals. Scope and Target Audience This report has been prepared for the assessment of individuals who may have had risky contact with a measles case, the implementation of PEP, and the management of follow-up processes. It aims to provide a supportive resource for both clinical practices and public health processes. The primary target audience of the report is healthcare personnel responsible for the assessment and management of individuals who have had contact with measles. In this context, primary care providers, pediatricians, infectious disease specialists, emergency department physicians and nurses working in hospitals, infection control teams, epidemiology and surveillance teams working in provincial and district health directorates and public health units, and healthcare personnel working in collective living areas such as schools and daycare centers can be considered target users of the report. Measles Transmission Measles spreads through airborne droplets or direct contact with respiratory secretions from an infected person (10). The basic reproduction number (R₀) for measles is reported to be 12-18. This high value makes measles one of the most contagious infections known, indicating the average number of people who can be infected by a single case in a community where no one has had measles before or gained immunity through vaccination (Figure 1) (11). The measles virus can remain active and infectious in the air and on contaminated surfaces for a certain period of time after an infected person leaves an enclosed environment, potentially leading to disease development (1,5). Experimental studies have shown that measles virus RNA can be detected in the air and on surfaces in patient rooms. Limited systematic data suggest that virus particles can remain airborne for approximately 30-120 minutes, particularly under low humidity conditions. These findings support the general acceptance in public health guidelines that the virus can remain infectious
through the air for up to two hours after the infected individual leaves the enclosed environment. Therefore, individuals who share the same environment for a short period of time are also considered to be at risk for measles (12,13). The incubation period for measles is generally 10-14 days from exposure to the measles virus until the first symptoms appear. Symptoms seen in the early period are mostly characterized by fever, cough, fatigue, conjunctivitis, and runny nose. The incubation period can be as short as seven days, but rarely extends up to 23 days. However, in outbreak control strategies involving quarantine, isolation, and contact tracing, the incubation period is practically considered to be from 7 to 21 days (1-3 weeks) after exposure (1,7). The aim of keeping the isolation period short and long, considering the most exceptional cases from the 7th to the 21st day after contact, is to reduce the risk of measles transmission to the lowest possible level, even to zero. This is summarized in Figure 2. Contagiousness begins four days before the onset of the rash and continues for four days after the rash appears. In immunocompromised individuals, the viral shedding period may be prolonged, and contagiousness may persist throughout the entire duration of the clinical illness (7,10). A general summary of the development of the clinical picture of measles and its complications is also attempted in Figure 3. Risk Groups Individuals who are unvaccinated, incompletely vaccinated, or have not previously had measles are considered to be at high risk for measles (1,7). In addition, certain specific groups are more likely to experience severe, atypical, and complicated forms of the disease. In immunocompromised individuals, especially those with T-cell dysfunction, measles may be asymptomatic, the disease may present with a prolonged clinical course, and viral shedding lasting for weeks after the acute phase may be observed (14). Malnourished children, especially those with vitamin A deficiency, are at risk for severe disease and complications. It has been reported that complications related to measles are more common in children under five years of age and adults over twenty years of age (7). Measles infection during pregnancy can lead to serious consequences for both the mother and the fetus, and it is associated with an increased risk of premature birth, spontaneous abortion, and low birth weight babies (15). However, a definitive causal relationship between measles virus infection and congenital anomalies has not been established. Healthcare workers, on the other hand, pose a risk both to themselves and to the patient population they serve if they do not have acceptable proof of immunity (16). Therefore, timely administration of measles-mumps-rubella (MMR) to healthcare workers plays a critical role in preventing outbreaks in healthcare facilities and communities.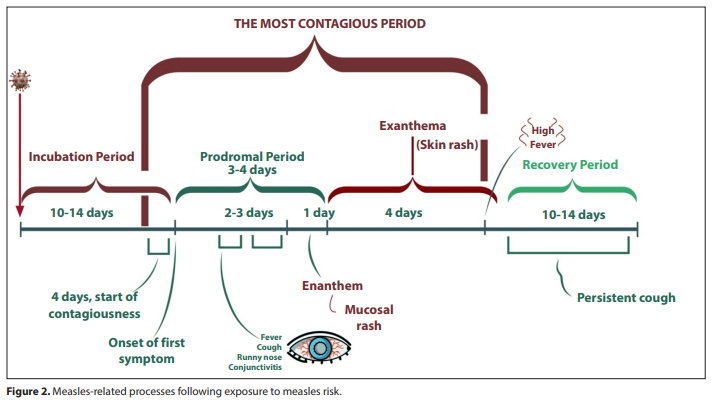
Definition of Contact A measles contact is defined as a susceptible individual who has had epidemiological contact with a measles case (laboratory or clinically diagnosed) or a suspected measles case until proven otherwise, during the infectious period, in a manner that could lead to transmission of the virus. Epidemiological link covers contacts occurring between four days before the onset of rash and four days after the onset of rash (5). It is important to note that the four-day period after the onset of rash applies to individuals who were healthy prior to this period. In cases of non-immunity, this period may extend throughout the rash and even beyond. In national field applications, contacts are defined as household members, individuals sleeping in the same environment, individuals in the same classroom or workplace, individuals in the same area as the case in healthcare facilities, and individuals traveling in close proximity on public transportation (9). To elaborate on this general definition and establish a practical framework for the concept of contact in practice, the situations considered to be risky contact for measles by the Pediatric Infectious Diseases and Immunization Society are summarized below. Contact at Risk for Measles: • All individuals living in the same household as the case, • Individuals sleeping in the same environment as the case (e.g., hospital wards, boarding schools, military units), • Those who share the same classroom or school with the case, • Children and adults receiving daily care services in the same place as the case, • People who share the same waiting area or examination room in healthcare facilities or who enter these areas within two hours after the case leaves, • Work colleagues who work in the same workplace as the case, • People who shared common areas by being in the same work or educational unit as the case, • Among passengers traveling on the same flight as the case, people sitting in the same row or two rows in front or behind (this approach represents the most frequently risky position due to airflow and cabin structure in modern aircraft. However, given the high contagiousness of measles and factors such as movement within the cabin, it should be considered that all passengers on the flight may potentially be at risk, and a broader contact assessment should be conducted when necessary, taking into account the duration of the flight), • Other individuals who were present in the same time frame in the common areas where the case was located (such as cinemas, shopping malls, restaurants, public transportation vehicles).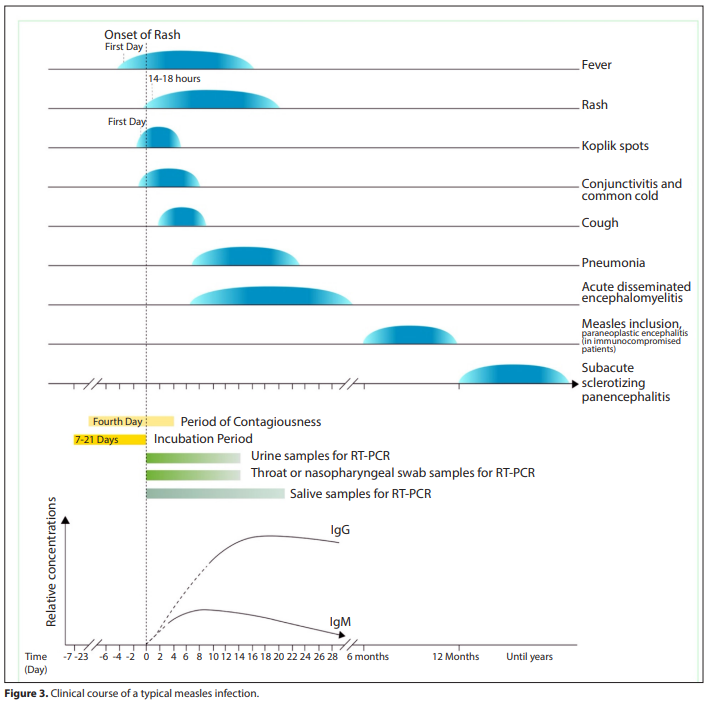
Among those at risk of exposure, it is important to prioritize groups that are at high risk of developing severe measles and that could contribute to secondary spread of the infection (1,7). In this context, unvaccinated or immunologically compromised infants and children, immunocompromised individuals, pregnant women, and healthcare workers are among the priority contact groups (8). Contacts in schools, daycare centers, and similar communal living areas require early assessment and intervention due to the frequent and close nature of their contact (8,10). Contacts occurring in healthcare settings are of particular importance due to the presence of vulnerable patient groups and the potential for intense contact; the rapid identification and management of contacts identified in these settings is considered critical for outbreak control (8-10). In these groups, early intervention based on risk assessment may be necessary without waiting for the clinical picture to become clear.Immunity Against Measles and Its Evidence Natural measles infection generally results in lifelong immunity (17). Two doses of measles vaccine administered at the appropriate time during childhood achieve seroconversion in 95-97% of the cases, and this immunity is considered to provide long-term protection against all known measles virus genotypes (18). Appropriate vaccination or full measles vaccination coverage refers to two doses of measles vaccine administered after the baby’s first birthday, with at least four weeks between doses, and administered according to the recommended schedule. However, data obtained in recent years show that in communities where natural measles virus circulation has been interrupted, vaccine-induced immunity may decrease over time due to the loss of the “booster” effect, as there is no exposure to measles to naturally re-stimulate immunity. It has been reported that this situation may lead to the development of renewed susceptibility, particularly within approximately 10 years, and may pose a risk of outbreaks even in areas where measles elimination has been achieved (11,19). This situation should be kept in mind when evaluating cases, but it should generally be accepted that those who have received two documented doses of vaccine are protected for life. Findings suggesting that this risk has emerged in regions that have achieved elimination targets include an increase in reported measles cases among individuals who have received two doses of vaccine, a shortening of the duration of transplacental passive immunity passed from vaccinated mothers to newborns, and the occurrence of measles cases in adult age groups that were previously thought to be largely protected during national epidemics (19,20). The age at which the measles vaccine is administered is one of the key factors determining the strength of the immune response. Vaccination before or around six months of age may not result in the desired level of serological response due to the immune system not being sufficiently mature and the suppressive effect of neutralizing antibodies passed from the mother (21). The proportion of children who achieve protective antibody levels after measles vaccination is approximately 85% at nine months of age, rising to 95% at 12 months. In children younger than nine months, the likelihood of developing lasting protective immunity is also lower due to the presence of maternal antibodies and incomplete immunological maturation (21,22). Therefore, vaccinations administered after 12 months (after the child’s first birthday) should be considered a full dose of the vaccine. Therefore, administering the first dose of the measles vaccine at 12 months (in some countries, the first vaccine is administered at 15 months) provides a higher level of protective immunity; however, single-dose administration is only possible in areas where the risk of measles is very low. The high level of community immunity required to stop the circulation of the measles virus cannot be achieved with a single-dose vaccination program. The first dose can achieve a 95% seroconversion rate. The administration of two doses of measles vaccine is considered a fundamental public health requirement to ensure that individuals who do not respond to the first dose are also immunized and that protection lasts for life (11,22). The term “adequate vaccination” or “fully vaccinated against measles” refers to a two-dose measles vaccine administered in the recommended manner, with the first dose given after the baby’s first birthday, followed by a second dose at least four weeks later. During the contact tracing process, accurately determining each contact’s immunity status to measles forms the basis for contact management and PEP decisions. During this assessment, the concept of “proof of immunity to measles” should be used as a basis, and contacts should be classified as susceptible or immune accordingly. In the absence of evidence of immunity to measles, contacts should be considered susceptible and evaluated for PEP. Evidence of immunity to measles is accepted with documentation of at least one of the following (1,5,23,24). • A record of a live attenuated (weakened) measles vaccine administered at the appropriate age (the first dose administered after 12 months of age and the second dose administered at least four weeks after the first dose in children older than 48 months) is one of the accepted proofs of immunity. In practice, at least one dose of measles vaccine administered after the age of one in preschool children is considered sufficient. Two doses of vaccine are required for school-aged children between kindergarten and 12th grade; the first dose must be administered after the age of one, and the second dose must be administered at least four weeks after the first dose. • In adults who are not at high risk (here, risk should be assessed based on both underlying disease and the characteristics of the people they regularly come into contact with), a single dose of measles vaccine administered after the age of one can be accepted as proof of immunity. For high-risk adult groups such as university students, healthcare workers, caregivers, teachers, and international travelers, two doses of vaccine are required; the first dose should be administered after the age of one, and the second dose should be administered at least four weeks after the first dose and should be documented. • Immunity to measles can also be documented by laboratory tests. Serological test results showing the presence of protective levels of antibodies against the measles virus are accepted as proof of immunity. For measles, an IgG antibody value of ≥120 mIU/mL measured by the ELISA method is considered protective, while <120 mIU/mL is not protective. In tests where ELISA results are reported as an index (S/CO), there is no universal biological threshold; positivity and cutoff values are defined according to the cutoff values specified by the manufacturer of the commercial kit used and validated against reference methods; the classification ≥1.1 positive, 0.8-1.1 borderline, and <0.8 negative is frequently used in the literature (25,26). • The presence of reliable medical records indicating previous measles infection is also considered evidence of immunity. While these records may include a physician’s diagnosis, it is preferable that they be supported by laboratory findings. Protection status against measles; • The presence of two doses of vaccine, • Serological detection of antibodies, • Documented history of previous measles infection. Post-Exposure Prophylaxis Options Measles PEP encompasses different intervention options that can be applied to prevent infection in susceptible individuals who have been in contact with a case and to control the spread of measles. These options are: • Administration of a live attenuated measles vaccine after exposure, • Administration of measles IG or standard IG after exposure, The prophylaxis approach is determined by considering the timing of exposure, the age and immune status of the exposed individual, as well as special risk factors such as pregnancy, immunodeficiency, and infancy. In this context, the main options that can be implemented within the scope of PEP are presented below. Vaccine Prophylaxis (Active Immunization) It is known that administering the measles vaccine within the first 72 hours after exposure to the measles virus provides protection in unvaccinated or incompletely vaccinated individuals (27). Even if infection develops in individuals vaccinated within this timeframe, it has been reported that the disease may be milder and the duration of symptoms shorter (1,10). Current literature strongly supports the effectiveness of post-exposure vaccination. A comprehensive systematic review covering studies published after 1970 reported that the effectiveness of post-exposure vaccine prophylaxis ranged from 83.4% to 100% (8). Vaccines administered after 72 hours are not considered effective for PEP; however, if a vaccine is planned to be administered as part of the routine immunization program, it can be administered up to the 5th day (10). The measles vaccines currently in use contain live attenuated virus. These vaccines may be administered as a single-component measles vaccine or as a MMR or measles-mumps-rubella-varicella (MMRV) combination. It is accepted that all measles vaccines approved by the WHO provide a similar level of protection against natural measles virus genotypes and can be used interchangeably in immunization programs (24). There is no evidence that vaccinated individuals transmit the virus to others as a result of vaccination (28). The preferred vaccine for PEP is the measles-mumps-rubella vaccine. If this is not available, a single measles vaccine may also be used. MMR should not be preferred. Following vaccination, transient IgM antibodies develop in the blood and IgA antibodies develop on mucosal surfaces, while the IgG antibody response, which provides long-term protection, develops. Neutralizing antibodies against hemagglutinin (H) and fusion (F) proteins, in particular, are considered the most reliable indicator of protective immunity, with a level of >120 mIU/mL defined as the protective threshold (25). The standard dose of the measles vaccine is 0.5 ml and is preferably administered subcutaneously (under the skin). Although the vaccine is not recommended during pregnancy due to its theoretical risk, accidental administration does not require termination of the pregnancy (29). During the first six months of life, the measles vaccine should not be administered before six months of age due to the presence of maternal antibodies and the inability of the immune system to respond adequately to live attenuated vaccine. The vaccine is contraindicated in individuals with a known history of life-threatening allergy to vaccine components (e.g., neomycin or gelatin) and in pregnant women. Additionally, it is contraindicated in individuals with cellular immunodeficiency, hypogammaglobulinemia, severe immunosuppression, and/ or symptomatic HIV infection (CD4+ T lymphocytes <15% at any age; CD4 <1500 in <12 months, CD4 <1000 in 1-5 years, >5 years of age CD4 <500), leukemia, lymphoma, and other malignancies, high-dose immunosuppressive therapy (corticosteroids, chemotherapeutic agents, biological agents), and solid organ or stem cell transplant recipients should not receive measles-containing vaccines (1,10). Immunoglobulin Prophylaxis (Passive Immunization) IG are blood products used to provide passive immunity in situations where the measles vaccine is contraindicated or where the effective period of the vaccine (the first 72 hours) has passed (1). They should be administered within the first six days after exposure, with the highest level of protection achieved when administered within the first three days (7). PEP with IG is recommended, particularly in the following groups: • Infants younger than six months, • Pregnant women without evidence of immunity, • Individuals with severe immunodeficiency, and • Individuals for whom vaccination is contraindicated (1).Although the effectiveness of modern IG preparations is controversial due to plasma donors having vaccine-induced immunity rather than natural infection, a recent meta-analysis conducted in 2025 covering a total of 660 patients showed that IG prophylaxis is 76% to 100% effective in preventing infection, despite a decline in donor antibody titers (8). This analysis reported that infection rates in groups receiving IG remained between 0% and 30%. Data reported from Türkiye also support these findings. In a study by Caymaz and colleagues involving 187 infants, it was reported that 99% of infants who received intravenous immunoglobulin (IVIG) after high-risk exposure did not develop measles (30). IVIG is administered at a standard dose of 100-400 mg/kg. When administered prior to exposure, it is considered protective for three weeks following administration and sufficient to provide protection against exposures occurring during this period (1). If there is a possibility of exposure occurring more than three weeks after IVIG administration, an additional dose should be considered. IVIG is not routinely recommended for PEP in patients not already receiving IVIG therapy (7). However, studies show that IVIG is preferred in both immunocompetent and immunocompromised patients when intramuscular IG (IMIG) is not available (1,5,7). Due to the lack of access to IMIG preparations in Türkiye, IVIG is the primary prophylaxis method. The standard IVIG dose for high-risk infants and immunocompromised patients is 400 mg/kg (0.4 g/kg) (5,7). While standard guidelines recommend prophylaxis for the first six days, Turkish data show that administration on days 6-10 also provides protection and does not differ statistically from the first six days (24). In light of this information, the Pediatric Infectious Diseases and Immunization Society accepts that PEP can be administered up to the 10th day in premature infants, infants younger than six months at increased risk of measles complications, and pregnant women known to be susceptible to measles. IMIG is widely used worldwide. The standard dose is 0.25 mL/kg, with a maximum of 15 mL (1). The recommended dose for immunocompromised patients is 0.5 mL/kg (1,10). Due to its limited availability in our country and our greater experience with IVIG, the Pediatric Infectious Diseases and Immunization Society prioritizes the recommendation of IVIG. Subcutaneous immunoglobulin (SCIG) has been in use since 2006 and has similar indications to IVIG, eliminating the need for intravenous access. SCIG is administered once a week via subcutaneous infusion using a pump at a rate of 15 mL/ hour; but for volumes exceeding 15 mL, different application sites are used. The recommended dose range is 100-200 mg/ kg, and multiple consecutive weekly doses may be required to achieve protective antibody levels. It is generally preferred as maintenance therapy in patients already receiving IVIG (1). Measles-specific IG has been used to provide passive immunity when administered within the first six days after exposure to prevent the disease or reduce its severity; however, it is no longer produced or available and is not used in clinical practice today. Measles antibody titers in IG products are an important variable affecting the success of prophylaxis. It has been shown that the rate of prophylaxis failure increases in batches with low antibody concentrations, while complete protection is achieved in batches with high concentrations (31-33). High-volume IVIG administration (400 mg/kg) can tolerate the deficiency that low antibody titers may cause (8,31). Due to the risk of passive antibodies neutralizing the live vaccine virus, measles-containing vaccines (MMR, MMRV, or MMRV) should be administered at least 6-8 months after IVIG administration (at least six months after IMIG and at least eight months after IVIG) in individuals receiving IG (1,10). Evaluation of the Source The assessment of the source should be initiated by clarifying the onset of symptoms, epidemiological history, infection history, and contact history; suspected cases should be rapidly identified for surveillance purposes without waiting for laboratory results. If the case is in another province, inter-provincial reporting procedures should be applied, and interviews and public health follow-up should be conducted in coordination between the relevant units (1,34). The vaccination status of the case, including dates, should be checked, and the results of relevant laboratory tests should be confirmed, or it should be confirmed that appropriate tests have been requested and samples have been sent to the laboratory as a priority. To accelerate public health intervention, the laboratory should report the results by telephone to the relevant authority when urgent results are required, or active contact with the laboratory should be ensured (9). The possible exposure period and infectious period should be determined, and the source of infection should be identified. During this process, the patient’s travel history, contact with a confirmed case during the infectious period, or recent contact with individuals who have had a fever/rash illness consistent with measles should be investigated. In addition, a chronological list of possible contacts should be compiled, and the locations where the case may have been infectious should be identified. These locations may include daycare centers and schools, workplaces, public transportation, stores, cinemas, clinics, hospital emergency rooms, and laboratory specimen collection centers (1,7). Case management should be comprehensively reviewed, and appropriate isolation measures should be implemented. Particularly in hospitalized cases, it must be ensured that infection control practices are fully implemented (1,9).Post-Exposure Prophylaxis Practices In measles, PEP is administered to prevent the development of the disease in susceptible individuals or to reduce its clinical severity. When selecting a prophylaxis method, the time elapsed since exposure, the individual’s age, immune status, and whether they belong to a high-risk group must be evaluated (7,10). General principles: In exposed individuals, evidence of immunity to measles should first be sought. Individuals without proof of immunity or with an uncertain immune status should be considered susceptible. The time elapsed since exposure is decisive in selecting the prophylaxis method: Vaccination and/or IG can be administered within 0-72 hours after exposure; only IG is administered between 72 hours and six days; if more than six days have passed, prophylaxis is normally ineffective and monitoring is applied. In individuals found to have no immune response to measles, if no clinical measles symptoms develop, the MMR vaccine should be repeated at an appropriate time (at least four weeks later if only the vaccine was administered, or 11 months later if IG was administered) (1,7,10). In individuals aged 12 months and older who have never been vaccinated or have received only a single dose, a single dose administered within the first 72 hours after exposure (at least four weeks after a single dose of MMR vaccine if given) can prevent MMR disease. The recommended prophylaxis algorithm according to the age of the exposed individual is shown in Figure 4. PEP in special groups: Pregnant women, infants <12 months, immunocompromised individuals, and healthcare workers are groups with a different risk profile than the standard population; therefore, specific prophylaxis approaches and application periods have been determined for each group. Recommendations for these special situations are summarized below. • PEP in pregnant women: Since live vaccines are contraindicated during pregnancy and in women suspected of being pregnant, MMR vaccination is not recommended as PEP. The serological immunity status against measles should be assessed in all pregnant women. In pregnant women without proof of immunity or whose immunity status cannot be determined, IVIG (400 mg/kg IV) or IMIG (0.5 mL/kg; maximum 15 mL) is recommended within the first six days after exposure (10,24). • PEP in infants <6 months: Prophylaxis after measles exposure in infants varies according to age and immune status. Infants younger than six months are considered unprotected and IG is administered (7,10). • PEP in infants aged 6-12 months: In unimmunized infants aged 6-12 months, the MMR vaccine can be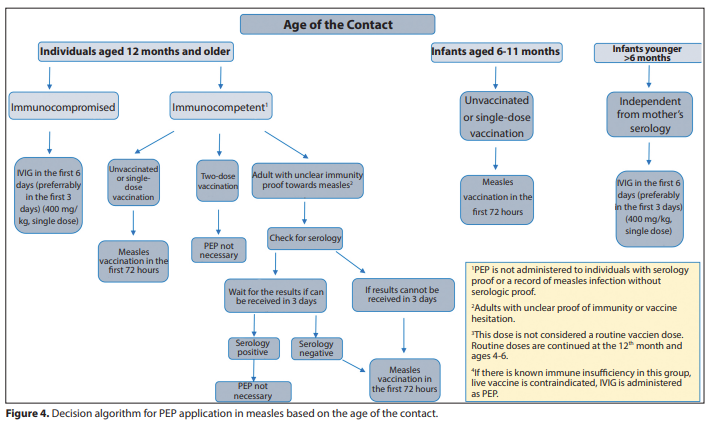
administered as an early dose within the first 72 hours after exposure; if the vaccine cannot be administered, IG is preferred. Infants who receive the early dose of MMR continue to be vaccinated according to the routine vaccination schedule (7,10). • PEP in premature infants: Premature infants are vulnerable to measles in the early stages of life due to the rapid decline of measles antibodies passed from the mother. Studies show that these antibodies generally lose their protective effect between 3-6 months (34). Therefore, additional protective measures are necessary following measles exposure in premature infants. Some international guidelines recommend the use of IVIG or IMIG as PEP in premature and infants younger than six months. Particularly in preterm infants younger than six months, post-exposure administration of IVIG (400 mg/kg) or IMIG (0.5 mL/kg) is recommended. Administration of IVIG within the first six days after exposure, preferably within the first three days, provides a high level of protection (35). Studies report that the incidence of measles in infants receiving IVIG is less than 1-2%, with no serious side effects observed (36). In infants older than six months without immunity, the MMR vaccine can be administered within the first 72 hours after exposure. However, data on the immunogenicity and safety of the vaccine in premature infants are limited (37-39). • PEP in immunocompromised individuals: Live vaccines are contraindicated in individuals with hematologic malignancies, organ transplant recipients, and those receiving heavy immunosuppressive therapy. IG is preferred for PEP in this group (10). Since IVIG is considered protective for approximately three weeks when administered at doses of 100-400 mg/kg, the need for additional prophylaxis in individuals receiving regular IG should be determined on an individual basis, based on the time of the last administration. • PEP in healthcare workers: Healthcare workers with evidence of immunity to measles do not require PEP or work restrictions; however, they should be monitored for symptoms for 21 days from the date of last exposure. Healthcare workers without evidence of immunity require work restrictions even if they have received PEP. Healthcare workers with suspected or confirmed measles should not go to work from the prodromal period until the end of the 4th day after the rash appears. For immunocompromised workers, this period should continue until the disease is completely resolved due to prolonged viral shedding (5,7). Follow-up and Monitoring Post-exposure follow-up is critical for breaking the chain of measles transmission and detecting potential secondary cases early. All contacts should be closely monitored, regardless of whether prophylaxis has been administered (1). The physician who first identifies and reports the case is responsible for this follow-up, as well as for coordinating reporting and PEP implementation. Individuals who remain asymptomatic during the monitoring period are considered healthy; susceptible contacts and their parents or caregivers should be informed about the risk of infection. It should be emphasized that atypical measles symptoms may develop even in individuals who have received the vaccine or IG, and the course of the disease may be unusual (1,5,7). Routine MMR vaccination planning should be carried out for unimmunized individuals; unimmunized individuals who have received IG and PEP should complete the MMR vaccination at least six months after IMIG and at least eight months after IVIG, if they are over 12 months of age (10). All follow-up forms should be archived regularly and forwarded to the public health unit (9). Symptoms to monitor: The main symptoms to monitor in exposed individuals are fever, cough, maculopapular rash, runny nose, and conjunctivitis. It should be noted that these symptoms may appear within 7-21 days after the last infectious day of contact. If any of these symptoms appear, the person should be immediately isolated and reported to the health authorities (1,5,7-10). Follow-up method: The follow-up process can be carried out through daily phone calls or face-to-face checks. Family members or caregivers should be informed about the regular reporting of symptoms. During the follow-up period, it is recommended that contacts avoid entering public areas. If necessary, a home visit for medical evaluation may be requested, or authorities should be notified in advance before visiting a healthcare facility (1,5,7-10). Detection of cases in educational institutions: If a confirmed measles case is detected among students or staff, susceptible contacts or their parents should be informed of the risk of infection and warned to be alert for measles symptoms for 7-21 days (28 days in IG areas) after the initial contact (1,5,10). Criteria for returning to school or work: Susceptible individuals who receive the measles vaccine within 72 hours of initial exposure or IG within six days may return to work or school immediately, considering the potential for transmission to at-risk groups. If the vaccine is administered after 72 hours, individuals should be excluded from the work or educational setting for 21 days due to the risk of transmission. Those without symptoms may return to work or school after completing this period. In addition, the second dose of the measles vaccine should be administered at least 28 days after the first dose (1,5,8-10). Follow-up after exposure for healthcare workers: Healthcare workers with evidence of immunity do not re-uire PEP or work restrictions; however, they should be monitored for symptoms for 21 days from the date of last exposure. Healthcare workers without evidence of immunity should receive prophylaxis and be excluded from work between the 5th day after the first exposure and the 21st day after the last exposure. Healthcare workers with suspected or confirmed measles should not go to work from the onset of prodromal symptoms until the end of the 4th day after the rash appears. Since virus shedding may be prolonged in immunocompromised workers, the return-to-work period should be extended until complete recovery (1,5,8-10). Exceptions and special circumstances in monitoring: A susceptible person may return to work under supervision if they are in a work environment without contact with at-risk groups. During this period, symptom development should be monitored through daily telephone or face-to-face follow-up, and clinical evaluation should be performed if necessary (1,7). Quarantine and restrictions: The duration and scope of quarantine depend on the individual’s susceptibility to measles, whether MMR vaccination has been administered, and the timing of administration. Individuals not under quarantine should avoid contact with children under 12 months of age or unvaccinated children, pregnant women, immunocompromised individuals, and healthcare facilities for 21 days (19). Public health follow-up: Provincial Health Directorates or Public Health Directorates are responsible for coordinating contact tracing. If a cluster of cases is suspected in the community, field studies should be conducted and additional measures planned (9). Implementation and Logistics PEP is necessary in appropriate indications; however, its implementation is costly and logistically challenging (8). In our country, there is currently no Health Practice Regulation covering the use of IVIG or SCIG in measles PEP. Therefore, in situations where IG administration is required, physicians must prepare the relevant drug reports within the existing legal framework, considering the patient’s benefit. It would be appropriate to establish official regulations in this area. Since there are also limitations in accessing other types of IG in our country, IVIG is currently preferred. In situations where prophylaxis should be administered with vaccines, the measles vaccines currently available in our country are MMR and MMRV vaccines. The literature shows that the risk of transmission is lower in individuals with secondary vaccination deficiency (new cases). Therefore, public resources will be more effective when used primarily in unvaccinated individuals and groups with primary vaccination failure (8). Rapid diagnosis, accurate reporting, and a well-structured surveillance system are essential for the effective implementation of prophylaxis and surveillance processes. An effective surveillance system should have clear definitions, be understandable and applicable by all healthcare workers, and be regularly evaluated at the national and regional levels. It is important that all healthcare institutions are integrated into this system and that the forms used are standardized and applicable. In the implementation of prophylaxis and surveillance, the responsibilities of the healthcare system tiers should be clearly defined. It would be appropriate to prepare a comprehensive action plan in which all physicians working in primary health care facilities and hospitals are actively involved. Ethical and Legal Dimension Measles is a disease subject to mandatory reporting in our country, and practices related to its reporting and case management are regulated by relevant circulars and regulations (40). In this context, healthcare institutions are obliged to immediately report cases to the relevant units and contact tracing and prophylaxis practices are carried out in accordance with legal requirements. Although the circulars and regulations published need to be updated, they are legally binding for all physicians in their current form. Contact tracing is required for every new case, even if it involves many contacts. However, managing the effects of exposure and the feasibility of this management pose significant challenges. In cases of contact occurring in areas far from large medical centers, rapid and timely intervention and access to prophylaxis products can complicate case management. Conclusion Measles is a disease that requires rapid and effective intervention after exposure due to its high contagiousness and risk of serious complications. The accurate identification of contacts, assessment of their immune status, timely application of appropriate prophylaxis methods, and implementation of systematic follow-up processes are critical in breaking the chain of transmission. Rapid reporting, comprehensive case assessment, contact tracing, and coordination of PEP applications are fundamental elements for controlling measles in both clinical and public health dimensions. In this context, current scientific evidence and national experiences show that a systematic and coordinated approach is the most effective strategy for preventing secondary cases and maintaining community immunity.