


ABSTRACT
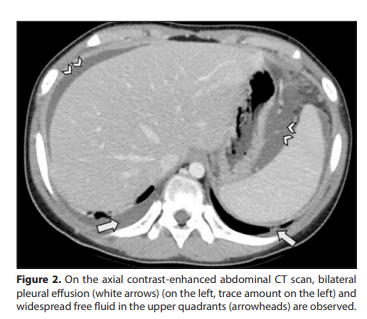
An 11-year-old girl presented to the pediatric emergency department with complaints of weakness, fatigue, drowsiness, abdominal pain, and intermittent fever reaching up to 38 degrees Celsius for approximately 10 days. Her history revealed loss of appetite and a history of eating cottage cheese. There was no history of vomiting, diarrhea, night sweats, joint stiffness, drinking raw milk, contact with animals, weight loss, tuberculosis exposure, rash, or photosensitivity. There was no burning sensation during urination or foul-smelling urine. Physical examination revealed abdominal distension and tenderness. The liver was palpated 6-7 cm below the costal margin, and the spleen was palpated 4-5 cm below the costal margin. Her temperature was measured at 37.9 °C. Laboratory tests showed an erythrocyte sedimentation rate of= 24 mm/hour (nodular lesions in the omentum, diffuse thickening of the peritoneum, enlarged lymph nodes at the mesenteric root, and pleural effusion in the lung bases included in the sections were detected (Figure 1-3). Peritoneal fluid was sampled by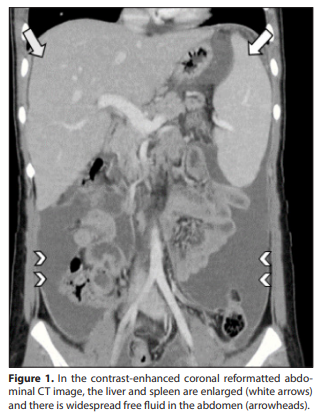
interventional radiology; fluid protein was= 5.6 g/100 mL (<3 g/100 mL), fluid lactate dehydrogenase (LDH) was= 330 IU/L (<200 IU/L), fluid LDH/serum LDH= 1.4 (<0.6), fluid albumin/ serum albumin= 0.8 (<0.5), adenosine deaminase activity= 42 U/L (<40) were detected, and 96% lymphocyte predominance was observed on direct examination. In histochemical studies of sputum, fasting gastric fluid, pleural effusion, and ascitic fluid samples collected on consecutive days, acid-fast bacilli were not detected, and no tubercle bacilli grew in cultures. A tru-cut biopsy was obtained from nodular lesions in the omentum by interventional radiology, and microscopic examination of the specimens reported the presence of numerous granulomas. Based on the patient’s history, examination, and radiological findings, what is your diagnosis? DIAGNOSIS: Tuberculous peritonitis Short discussion Abdominal tuberculosis is a rare form of extrapulmonary tuberculosis, and its clinical manifestations may present as acute, chronic, or acute exacerbation on a chronic background. The most commonly reported symptoms in various studies are fever, weight loss, fatigue, and abdominal pain. Abdominal tuberculosis can be transmitted hematogenously from the primary focus, by swallowing sputum containing the tuberculosis bacillus, by consuming contaminated milk or food products, or by direct spread from adjacent structures. Abdominal tuberculosis may involve the gastrointestinal system, peritoneum, lymph nodes, or solid organs; however, the most commonly affected areas are the peritoneum and abdominal lymph nodes (1,2).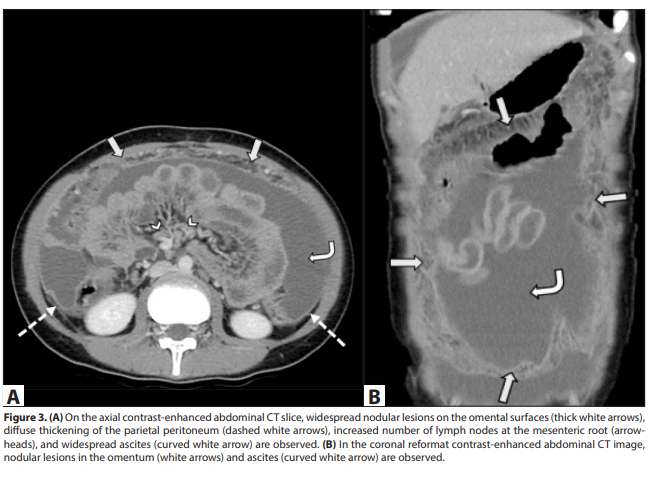
Peritoneal tuberculosis is a common subtype of abdominal tuberculosis. Peritoneal involvement is thought to develop either when the infection reaches the mesenteric lymph nodes (as a result of hematogenous or lymphatic spread) and ruptures into the peritoneal cavity, or as a result of direct spread along the serosa from adjacent structures (1,3). The demonstration of acid-fast bacilli in peritoneal fluid, and culture positivity have been reported rarely in the literature (1,3). In a series of 88 cases of abdominal tuberculosis, the rate of microbiological diagnosis was reported to be 11% (4). The likelihood of diagnosis based on microbiological criteria is low. Radiological examinations play a critical role in the diagnosis of peritoneal tuberculosis. US and CT are the most frequently used imaging methods for diagnosis. CT is more sensitive than US in evaluating changes in the peritoneal surfaces, mesentery, and omentum (5). Mesenteric and omental involvement is characterized by micro (5 mm) lesions or thickening of the mesenteric leaves and omental surfaces. A specific subtype of omental involvement is the “omental cake” appearance, which is characterized by widespread and coarse nodular thickening; in this case, peritoneal carcinomatosis should also be considered in the differential diagnosis. The most common findings in peritoneal involvement are diffuse or nodular peritoneal thickening. US may reveal peritoneal thickening, usually hypoechoic, 2-6 mm thick, and nodules smaller than 5 mm, and these findings become more prominent in the presence of ascites. On CT, marked contrast uptake in uniformly thickened peritoneum is typical. Ascites is seen in 30-100% of cases of peritoneal tuberculosis (5,6). US is more sensitive in detecting small amounts of fluid or loculated fluid. Fine septations, fibrin bands, and debris-containing appearances are common findings. On CT, ascites fluid typically shows high attenuation values (25-45 Hounsfield units), reflecting its high protein and cellular content. Chylous ascites is rarely seen, and in this case, a fat-fluid level may be detected. Three forms of tuberculous peritonitis have been described: The most common “wet” type is characterized by abundant, diffuse or loculated, viscous ascites. The “fibrotic-fixed” type is characterized by omental masses, adhered bowel loops, and mesenteric involvement. The “dry” type is characterized by caseous nodules and intense adhesions (5,6). In our patient, the imaging findings suggested tuberculous peritonitis. The diagnosis was confirmed by the presence of granulomas in the tru-cut biopsy of the omental nodules performed by interventional radiology, analysis of the peritoneal fluid, and a positive Quantiferon test. With combined antituberculosis treatment, the patient’s symptoms and radiological findings on follow-up US examinations regressed.