


ABSTRACT
World War I was one of the most devastating wars in history in terms of military, economic, and health impacts, leaving deep scars on the countries involved. The destructive impact of the war was as significant economically as it was in terms of human and skilled labor loss. The total cost of this war to Germany, Austria-Hungary, the Ottoman Empire, and Bulgaria was $60.643.160.000; the total cost to Britain, France, Russia, the United States, and other countries was $125.690.477.000. The total cost of the war to the entire world amounted to 186.333.637.000 US dollars (1). Although it is not possible to calculate the exact cost of this war, which lasted four years, it is estimated that the cost to the country was quite high, considering that the US dollar at that time was worth approximately 34 times its current value and its impact on purchasing power (2). When examining the historical process, it is seen that wars are not only conflicts between military forces; they also have lasting and profound effects on demographic structure, production capacity, and public health. Since the 19th century, the development of modern warfare technologies, mass mobilization practices, and prolonged frontline warfare have dramatically increased casualty rates. For example, in the Crimean War of 1853-1856, epidemics such as cholera and typhus claimed more lives than combat losses; similarly, in the American Civil War (1861-1865), the number of soldiers who died from disease exceeded combat deaths (3). The Franco-Prussian War of 1870-1871 and the Russo-Japanese War of 1904-1905 are examples of wars where losses intensified due to the increased firepower of industrialized warfare. This process demonstrates that wars were not limited to frontline combat; losses increased exponentially due to factors such as malnutrition, migration, epidemics, and the collapse of health infrastructure. Therefore, the high casualty rates seen in World War I should be evaluated as a continuation of the military and epidemiological experiences of the previous century (Figure 1). The Ottoman Empire, which was on the side of the Allied Powers during World War I, fought on the Caucasus (East), Iraq, Palestine-Syria, Gallipoli, Europe (Galicia, Macedonia, Romania), Yemen and Hejaz, Iran, and Libya fronts during this war, which also included the Gallipoli Victory, and it was one of the states that suffered the heaviest losses among the warring parties (Figure 1,2). During this period, agriculture, socio-economic production and distribution mechanisms, health infrastructure, and social order were severely shaken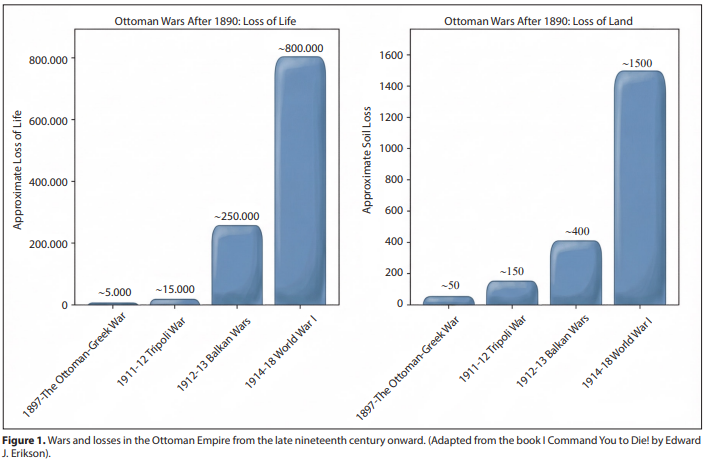

under the pressure of this large-scale, multi-front war, which the Ottoman Empire entered without sufficient preparation due to its constant involvement in wars, both materially and spiritually. Western Anatolia, the Balkans, and Eastern Anatolia were exposed to the migration of nearly 1 million refugees from the ongoing battlefields. This situation exacerbated the food problem in the region and led to serious loss of life due to the rise of cholera, typhoid, and especially typhus epidemics accompanying mass migration (4). In August 1914, the declaration of general mobilization led to a serious disruption of the economic structure in Ottoman territories, particularly in İstanbul. Under extremely challenging conditions of the period, various measures were attempted; although there was no quota system in place for security forces at the time, they restricted the purchase of more than one okka (1283 grams) of bread per person per day (5,6). On the other hand, drought, hail, floods, landslides, locust infestations, and epidemics continuously affected the population negatively (7,8). The combination of all these factors deepened the existing food shortage among the population, creating fertile ground for the spread of epidemics. Data for the two-year period following World War I shows that total losses, including those of the Allied and Central Powers, exceeded 37 million (9,10). This figure includes not only military casualties but also the devastating effects of epidemics on both military units and the civilian population. Considering that the total population of the Ottoman Empire in 1914 was 18.520.016, the magnitude of this loss becomes even clearer (11). Figure 3 shows the mortality rates of soldiers belonging to various states’ armies due to combat and epidemics, as published in a 1925 statistic in Paris. However, this study does not include any statistics related to the Turkish Army (12). The Ottoman Empire, still struggling to recover militarily, economically, and demographically in the aftermath of the Balkan Wars, sought to secure its safety within a large state alliance as the process of bloc formation in Europe accelerated. Following the agreement signed with Germany on August 2, 1914, the bombing of Russian ports in the Black Sea effectively drew the Ottoman Empire into the war; on November 11, 1914, war was officially declared on the Central Powers (Appendix 1) (Figure 4). Behind this decision lay the desire to preserve the territorial integrity of the empire, the desire to benefit from Germany’s military and technical support, and political goals such as the abolition of the capitulations (13). The Gallipoli Front was opened as a result of a strategic operation launched by the Central Powers to control the Straits, capture İstanbul, remove the Ottoman Empire from the war, 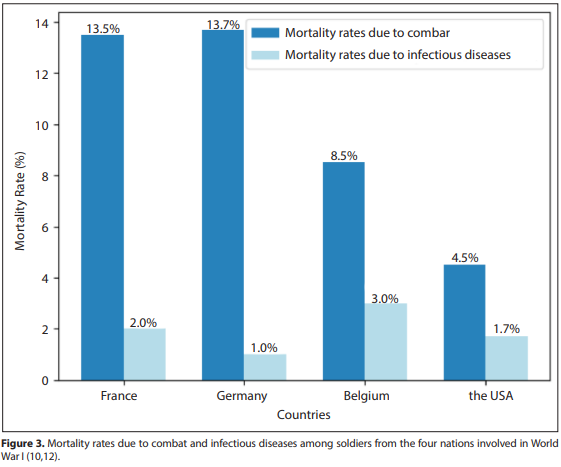
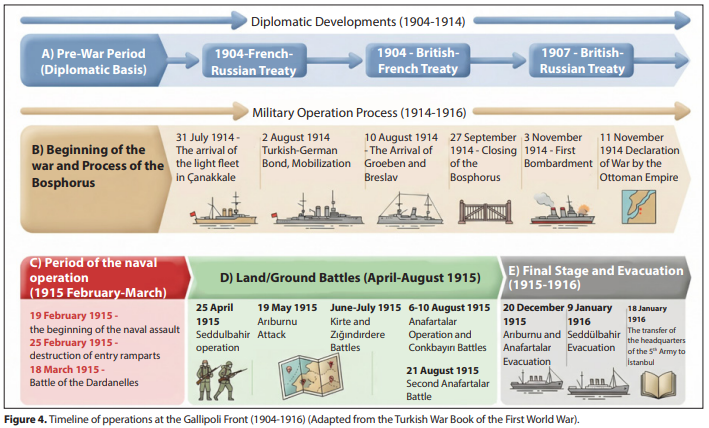
and open a secure supply line to Russia. The naval operation, which began on February 19, 1915, ended with heavy losses on March 18, 1915; this was followed by landings on the Gallipoli Peninsula on April 25, 1915. Throughout the Gallipoli Campaign, the Ottoman army suffered serious losses not only on the battlefield but also due to epidemics, malnutrition, and harsh environmental conditions. According to General Staff records, the total Ottoman casualties at the front (including martyrs, wounded, missing, and those who died of disease) were approximately 250.000. This situation clearly demonstrates the military and health devastation of World War I on the Ottoman Empire, particularly revealing the limitations of health services and logistical capabilities under multi-front war conditions (14). According to Ottoman State archive records, General Staff data indicates that the number of martyrs at Gallipoli was 57.263; the total casualties, including wounded, sick, and missing, reached 218.000 (13). Furthermore, according to Edward J. Erickson, the Ottoman Empire had 56.643 dead, 97.007 wounded, and 11.178 missing at the Gallipoli Front (14). Edward J. Erickson states that the Ottoman Empire’s losses in World War I were 175.220 killed in action, 61.487 wounded in action, 68.378 who died as a result of their wounds, 466.759 who died of disease, 145.104 prisoners of war, 303.150 disabled, and a total of 763.753 wounded (Table 1) (14). The total number of soldiers mobilized in the Ottoman Empire during World War I is reported to be 2.873.000 (14). According to a British source, in 1934, it was stated that the human losses of World War I could never be accurately calculated. The main reasons for this statement are said to be the inadequacy of statistics from countries such as Russia and Türkiye, France’s failure to publish the total number of wounded,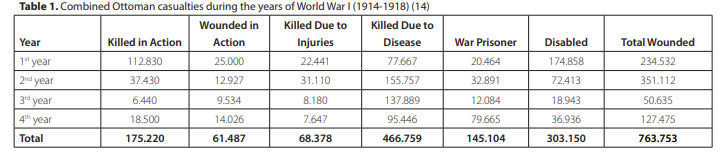
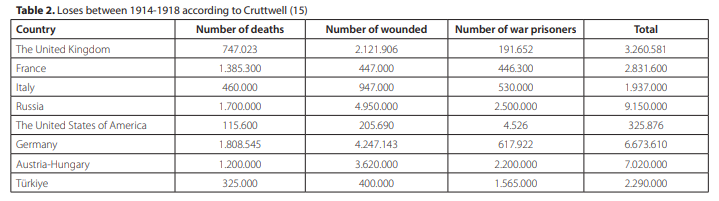
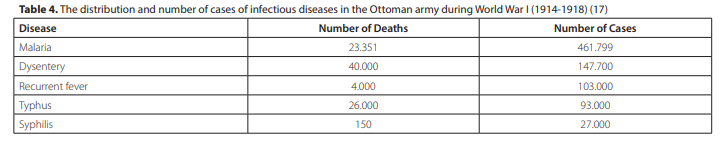
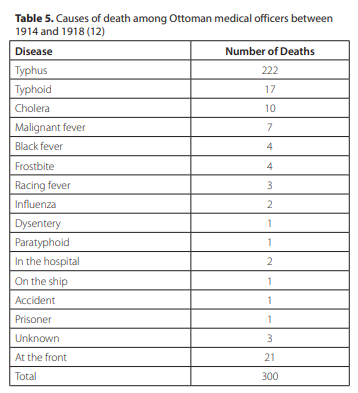
Germany’s failure to include the slightly wounded in its list of casualties, the fact that the number of casualties and prisoners of war in many countries is not known exactly, and the change of borders (12,15). According to British historian Cruttwell, the losses between 1914 and 1918 are listed in Table 2. However, considering the conditions of the war and the population of the period, it is understood that Turkish war losses were greater than those listed in Table 2. Furthermore, in 1943, Colonel A. G. Butler of the Australian Army pointed out that Turkish war casualties were higher (16). According to another source, the Ottoman Empire’s casualties over four years are given as estimated by the author (Table 3) (14). The number of soldiers who lost their lives in combat in the Ottoman Army during World War I is approximately 60.000, while the number of those who died due to epidemics is approximately 400.000. Furthermore, these figures do not include the losses incurred during the Gallipoli Campaign. According to the same source, the distribution of deaths by epidemic is shown in Table 4 (17). As can be seen from this distribution, mortality rates from typhus and dysentery are quite high (17). As a result of the increase in epidemics in the Ottoman army, medical officers were also affected, and medical personnel lost their lives due to epidemics (Table 5). During World War I, epidemics had a profound impact on the Ottoman Army; one of the fronts where deaths from epidemics were most prevalent was the Gallipoli Front (18). The Turkish army’s resources in terms of hygiene conditions were quite limited at the Gallipoli Front (12). The figures provided in the study published in 1940 by Prof. Dr. Tevfik Sağlam, who served as the Chief Medical Officer of the 3rd Army, confirm that deaths from epidemics in the Ottoman Army were quite high compared to other countries. According to this study, approximately 12% of the deaths in the German armies during the four years of World War I were due to epidemics, corresponding to a total of 177.162 people. This relatively low death rate in the German army was made possible by advanced accommodation and hygiene standards, as well as effective vaccination programs. Thus, the Germans managed to keep losses from epidemic diseases to a minimum. When these data are compared with the mortality rates in the 3rd Army, it is seen that disease-related deaths in the Ottoman Army were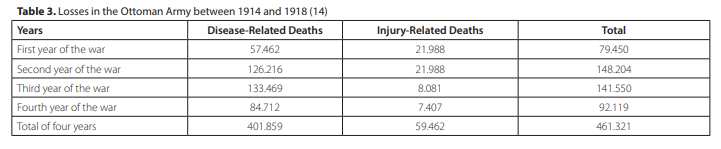
approximately 49 times higher than in the German Army (19,20). According to the Ottoman Army Medical Administration, 47% of enlisted soldiers serving in military units during the four-year war were hospitalized, and 17% of them died in hospitals (21). In addition to epidemics, there were also human factors affecting human health in the region. For example, the swampy areas east of Kumkale (Çanakkale) increased the mosquito population and the incidence of malaria among the local population and soldiers (12). Poor living conditions resulting from overcrowding in barracks, lack of or limited access to clean water in the forts, and difficulties in obtaining medicine in the region led to widespread health problems. Outbreaks of cholera, typhoid, and smallpox were frequent; diseases such as spotted fever (typhus), tuberculosis, pneumonia, and pleurisy (lung inflammation) were also seen. Another important factor contributing to the increase in infectious diseases was lice infestations. Furthermore, restrictions on the use of tincture of iodine due to iodine deficiency at the beginning of the war also led to more severe infections and made them difficult to control (21). In 1973, Ekrem Şadi Kavur assessed the situation at the Çanakkale Front as follows: “(...) During the Battle of Gallipoli, in a conversation I had with one of the wounded soldiers at the military school hospital [Mekteb-i Harbiye Hospital (Pangaltı/Harbiye, Şişli)] said that hell was on the Gallipoli Peninsula, meaning that it was surrounded by a ring of fire from the sea, air, land, and underground rat-sewer tunnels.” “Despite the concentration of large forces in a narrow area on the Gallipoli Peninsula, no major diseases other than malaria, dysentery, typhus, recurrent fever, and scurvy emerged. However, after the war turned into trench warfare, hospital cases began to increase.” (22). In the winter of 1914-1915, during the first phase of the war, a typhus epidemic, also known as spotted fever, was found to have spread throughout Anatolia. This situation made the conditions of war even more difficult, especially in Çanakkale and throughout Anatolia. Due to the harsh conditions created by the war and the spread of epidemics, in June 1916, in order to control the cholera epidemic in İstanbul, a compulsory vaccination program was launched for the public under the control of the Ministry of Health and based on the 3rd Addendum to Article 99 of the Penal Code, and various control mechanisms were established. Within this scope, bread distribution was limited to certain days and was only provided to individuals with a cholera vaccination certificate (23). However, the fact that the application was limited to İstanbul did not have a significant impact on conditions at the front (24-28). Mandatory cholera vaccination was discontinued in September 1919 with the end of the disease (23). Medical Activities at the Gallipoli Front The Battle of Gallipoli holds a special place not only for its significance in terms of military strategy and operations, but also for the medical practices developed under wartime conditions. During World War I, the Ottoman Army’s health services were carried out primarily by the General Inspectorate of Health, a high-level administrative and professional authority affiliated with the Ministry of War and responsible for the organization, supervision, and reporting of health services, as well as by military units at the corps, division, division, regiment, and battalion levels, as well as through field and mobile health institutions (29) (Figure 5). This structure consisted of the highest-ranking military personnel responsible for providing health services to the armed forces, as well as civilian physicians, dentists, pharmacists, and auxiliary health personnel assigned as needed (30). The duties and powers of the health inspectors were aimed at ensuring that health services were carried out in an orderly manner and in accordance with the regulations. In this context, any negligence detected in inspected areas and whether the medical officers acted in accordance with the regulations in force were reported; one copy of the prepared reports was sent to the local administration, and the other copy was sent to the center, namely the General Medical Directorate. In addition, the fight against infectious diseases such as syphilis, tuberculosis, malaria, and smallpox, as well as immunization practices, are regularly monitored to ensure they are carried out in accordance with the rules. Officials who are found to have abused their position, accepted bribes, or acted contrary to orders are reported to the center and asked to defend themselves. 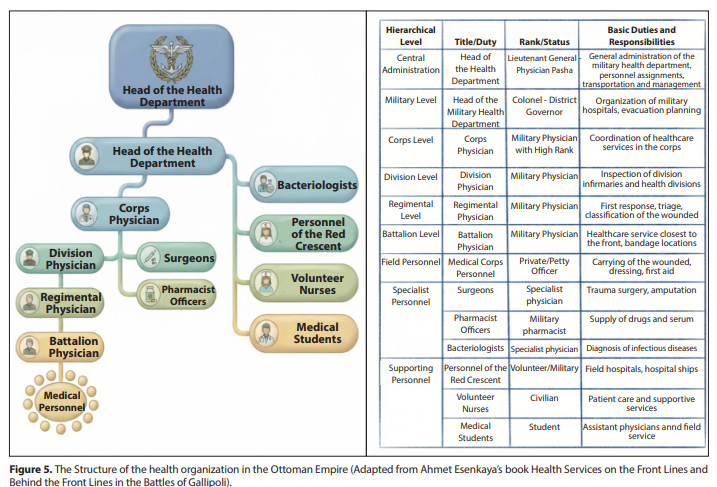
In addition, pharmacies, narcotic substances, and the activities of provincial health councils are also evaluated within the scope of supervision. Medical personnel were similarly distributed on the Gallipoli front, and throughout the war, health services were carried out by the 5th Branch Directorate (Chief Medical Officer) within the Gallipoli Fortified Position Command. In this system, the chief physicians of the Nizamiye and Redif divisions were responsible for supervising the implementation of health services belonging to the divisions, controlling health equipment, and gathering the wounded in health institutions (30). The chief physician of the Nizamiye division was the senior medical officer responsible for the medical services of regular and permanent military units, while the chief physician of the Redif division was the physician responsible for managing the medical organization of the reserve units formed during mobilization. The fundamental difference between them stemmed from the structure and organizational level of the units to which they were attached. After requesting medical drugs and dressing supplies, the Second Directorate of the Medical Department ensured that these requests were met by the nearest military hospital pharmacy, enabling the effective and sustainable provision of health services despite all the adversities of war (31). During peacetime, there were infirmaries with bed capacities ranging from 25 to 100 on the Gallipoli side in Seddülbahir, Kilitbahir, Maydos, and Bolayır, and on the Anatolian side in Kumkale and Çanakkale, under the command of the Fortified Position Command in the Çanakkale Region (29). There was also a 250-bed hospital in Çanakkale. According to the personnel and vehicle status table dated August 1, 1914, there were only eight medical personnel for 3.125 soldiers in the region. However, this situation changed with the start of the Central Powers’ attacks on the Dardanelles. New military units were dispatched to the region to defend the strait; in parallel, medical units were reinforced and the bed capacities of the infirmaries were increased (29). Following the defeat of the combined British and French fleets in the Battle of the Dardanelles on March 18, 1915, the defense of the Dardanelles Front was elevated to army level in line with the new circumstances; the units in the region were reinforced with new forces, and the 5th Army was established. The 5th Range Command was established to provide logistical support to the 5th Army; the management of health services was carried out by Medical Officer Lieutenant Colonel Dr. Mustafa Talat (Özkan), German Reform Commission Health Advisor Lieutenant Colonel Prof. Dr. Mayer, and Deputy General Inspector of Field Medical Services German Titri. By the end of June 1915, the 2nd Army had been deployed to the Seddülbahir region; responsibility for medical services was given to Chief Medical Officer Colonel İbrahim Tali (Uzgören) (13,30,32). In line with the course and developments of the Battle of Gallipoli, new hospitals and medical facilities were established to provide regular medical services to wounded and sick soldiers. In this context, the Darülfünun-ı Osmani Faculty of Medicine and the Gülhane Military Medical School, whose students were sent to the front lines, continued to serve as auxiliary war hospitals, limiting their educational activities (30). On April 25, 1915, with the landing operations of the Central powers, land battles began on the Gallipoli Front, and after this process, the casualty rates reached unexpected levels. The Central forces, which failed to achieve their objectives while suffering heavy losses, repeated the same attacks multiple times; however, each time, both sides suffered serious losses. Furthermore, the intertwined nature of the trench lines on the Gallipoli Front severely limited the mobility of the troops (33) (Appendix 2,3). During this period, which continued until September, there was a marked increase in the number of wounded, martyrs, and missing. According to sources, the total number of wounded during this five-month period was 86.857. Based on these figures, the average monthly number of wounded is estimated to be around 17.000. While the number of sick remained relatively low until August, it reached approximately 10.000 by August. After August 1915, although there was a decrease in the number of injuries in September, October, and November, there was a significant increase in the number of patients (30). As a result, this increase placed a heavy burden on the medical units and medical personnel worked intensively to cope with the increase in the number of wounded and sick (13). During the same period, sterilized towels were used in surgical interventions on the wounded; mixtures of boric acid, lemon salt, and warm water were used as antiseptics (34). Dead tissue in the wounds was removed with scissors, then cleaned using anesthetics and iodine, and the wounds were washed with pure hydrogen peroxide. As mentioned earlier, due to the shortage of iodine at the beginning of the war, extreme caution and economy were ordered in the use of tincture of iodine. Despite this, it is understood that infections played a major role among the causes of death seen after operations (34). During the Battle of Gallipoli, the Ottoman health organization was structured in a gradual and hierarchical manner, starting from the front line, extending to the rear, and then to hospitals within the country. First aid services at the front were carried out through field dressing stations and mobile hospitals; the wounded were then transferred to field hospitals after initial surgical intervention. Throughout the battles, the number of mobile and fixed hospitals operating behind the front lines was increased as needed, and a chain of evacuation for the wounded was established, concentrated particularly on the health units on the Gallipoli Peninsula and the Anatolian side (29). Field hospitals functioned as centers where wounded and sick personnel transferred from the front received more comprehensive treatment, underwent surgery, and where decisions on further transfer were made. These hospitals were organized under field inspectorates and provided services with both military medical personnel and a limited number of civilian doctors. However, personnel shortages, lack of medical supplies, and epidemics significantly limited the effectiveness of health services (35). The Ottoman Red Crescent Society (Kızılay) played an important role in alleviating the burden behind the front lines. The hospitals opened by the Society were organized both directly behind the front lines and in various cities in İstanbul and Anatolia as national hospitals. These hospitals undertook the long-term treatment of the seriously wounded, forming a semi-official health network supported by volunteer medical personnel and donations. Thus, a three-stage health referral and treatment system was established along the front-rangehome hospital line; despite the increasing number of wounded and sick during the war, an effort was made to establish a continuous health organization within the existing means (29). During the nine-month period at the Gallipoli Front, 110.220 wounded and 70.993 sick were transferred to field and home hospitals. Field hospitals were rear hospitals located in the field area (supply zone) following the first response units on the front line (field dressing stations, mobile hospitals, etc.) and were responsible for treating the wounded and sick who were evacuated from the front (30). They served as an intermediate level of healthcare between the front and the hospitals in the rear. During this period, although ten army and field hospitals were expected to operate with a staff of 95 physicians, these hospitals were only able to provide services with 61 physicians. Nevertheless, the existing bed capacity was increased from 3.000 to 10.000, and the number of hospitals was increased to 14. In these hospitals, 48.268 wounded and 22.619 patients were treated within nine months. 2.2% of the wounded (1.062) and 11.6% of the patients (2.623) lost their lives. Additionally, a total of 19.443 wounded were treated in the eight hospitals of the Red Crescent Society, which have a capacity of 5.450 beds, over a period of nine months (Figure 6) (28)
.At the Gallipoli Front, it was planned to treat lightly wounded, seriously wounded, and soldiers infected with contagious diseases in different hospitals, health services were carried out within this framework. The 5th Army’s health units were reinforced as the battle intensified, and on July 6, 1915, the total number of beds in the hospitals shown on the map (26 hospitals) reached 110.700 (Appendix 4) (13). Within this scope, the Akbaş and Eceabat (Maydos) hospitals played an important role in the transfer of wounded and sick personnel, while the Galata Hospital, with a capacity of 600 beds, was specifically allocated for the treatment of infectious diseases. Thus, thousands of wounded and sick were treated within a broad healthcare network encompassing field, mobile, Red Crescent, and local hospitals, within the available means (28). According to the data in archival documents, the total number of casualties at the Gallipoli Front was 251.447, consisting of 25.127 martyrs, 130.306 wounded, 10.867 prisoners and missing, 21.498 who died of disease, and 64.449 disabled (30). The loss figures in the table below are based on war records. These figures do not include losses during the naval warfare period (Table 6) (21). Diseases Reported at the Gallipoli Front and the Measures Taken A significant portion of the diseases observed at the Gallipoli Front were caused by limited access to clean water and inadequate nutrition and hygiene conditions. However, in May 1915, a serious malaria outbreak occurred in Kumkale and its surroundings. The intense breeding of Anopheles mosquitoes in the reed beds and marshes stretching from the Pınarbaşı spring to Kumkale was a decisive factor in the spread of the epidemic. Due to the inability to take effective and comprehensive measures under wartime conditions, the protective measures implemented were insufficient, and as a result, malaria-related deaths began to occur among the troops. Following two deaths that occurred within a short period of time in one of the units stationed in Kumkale, autopsies were performed, and microscopic examination of the spleen and heart blood samples revealed a high concentration of malaria parasites. Due to difficulties in obtaining effective drugs for malaria treatment, one gram of quinine was administered twice a week to the units serving in the region for prophylactic purposes. According to malaria statistics from 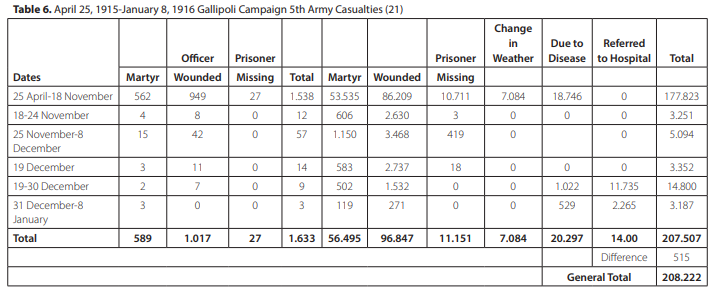
the 5th Army, 116.985 cases of malaria were recorded, resulting in 6.661 deaths. In addition, although rare, cases of relapsing fever caused by Borrelia recurrentis, transmitted by body lice, were also encountered. In this context, three mobile ovens and a range cleaning facility were put into operation, and the soldiers’ hygiene procedures were carried out in these facilities (21). Provisions sufficient to meet two months’ requirements were stored in the supply warehouses belonging to the 5th Army Supply Command. However, due to the inability to regularly supply units with foodstuffs such as meat, vegetables, and fruit that could not be stored, the soldiers’ diet was largely based on legumes. This situation led to an increase in health problems among the soldiers due to inadequate and unbalanced nutrition; in particular, a marked increase in cases of scurvy, characterized by gum recession and bleeding, associated with vitamin C deficiency, was observed. Sources indicate that approximately 1.000 soldiers showed signs of scurvy during the war. In response to these developments, a soldier’s daily food ration was officially determined under the “Rations and Feed Law” of September 12, 1914, with the aim of standardizing the military food supply system (35). According to this law, “a nutrition list consisting of 600 grams of flour, 250 grams of meat or 125 grams of roast meat, pastrami, sausage or canned meat, 86 grams of rice, 10 grams of oil, 20 grams of onion and salt” was created. Chickpeas, dried beans, vegetables, canned or fresh vegetables were to be provided in lieu of 1/4 of the meat. However, due to the prolonged war and the failure of shipments to reach the soldiers, the documents indicate a reduction in the soldiers’ rations (21). Another significant problem that arose during the war was outbreaks of diarrhea. The deepening of trenches after each air raid and the soldiers’ forced accommodation in damp, wet soil conditions led to the rapid spread of diarrhea cases among the troops. However, by temporarily removing soldiers from the trenches and improving hygiene conditions, the spread of the disease was largely brought under control (36). The insufficient hygiene of water sources used at the front caused a marked increase in cases of dysentery and cholera. Difficulties in obtaining medicines and medical supplies made it necessary to resort to alternative and supportive treatment methods under the existing conditions. In this context, clay soil applications were used for soldiers who contracted these infections (37). This substance, referred to in the literature as bolus alba or kaolin, was used in various countries as a supportive treatment element, especially during World War I, for diseases associated with intestinal infections. It is stated that kaolin’s adsorbent properties were utilized to reduce the frequency of defecation, particularly in cases of diarrhea and dysentery; in some applications, it was tried not only for therapeutic purposes but also for prophylactic (preventive) purposes. Indeed, Derek S. Linton’s study titled “War Dysentery and the Limitations of German Military Hygiene during World War I” states that similar supportive treatments were used in the context of the limitations of military hygiene practices under war conditions (38). Within the scope of preventive health practices, various measures were taken against the factors causing the spread and transmission of diseases such as malaria and typhus. In this context, importance was given to soldiers’ personal hygiene; drinking water was kept clean, toilets were regularly disinfected, and taps were installed on water containers (36). Despite all of these measures, it is understood that infectious diseases such as malaria, cholera, smallpox, and typhus continued to be seen at the front. In addition, diseases such as typhus, tuberculosis, pneumonia, and pleurisy were also prevalent (12). Protective measures were taken to prevent diseases seen at the front, such as vaccinating soldiers, disinfection and decontamination procedures, the use of ovens, and lighting fires to protect against mosquitoes and lice. Furthermore, to prevent infectious diseases among soldiers at the front from spreading to other patients in hospitals and the general public, citizens living in certain areas, such as Lapseki, were forcibly relocated. Vaccination Practices at the Gallipoli Front (Vaccination Program) Health services at the Gallipoli Front were approached within the framework of preventive medicine rather than curative practices, and the fight for health was conducted accordingly. In this context, measures to prevent epidemics, including ensuring cleanliness and hygiene, providing adequate and balanced nutrition, and vaccination activities, were among the priority measures. Quarantine stations were established for vaccination programs and basic health training for soldiers (39). Quarantine stations were essentially health facilities established in coastal areas near major ports to quarantine ships carrying passengers and personnel diagnosed with infectious diseases during voyages, to implement necessary health measures, and to treat patients. During the war, soldiers were subjected to drill training at quarantine stations set up in different locations before being sent to the front; they were vaccinated against infectious diseases such as cholera, dysentery, and smallpox, and vaccination programs continued in the same manner at the front (Table 7) (39). Additionally, the ATASE archives contain a vaccination directive for the 5th Army (See Appendix 5) (39). The provisions of this directive are as follows: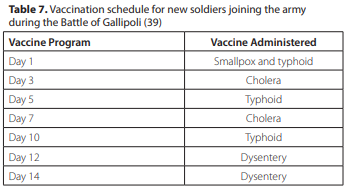
1. Vaccinations for smallpox, cholera, typhoid fever, and dysentery will be administered at the times specified below (Table 7) (39): 2. Procedure for administering vaccines to new recruits joining the army: 2.A. Schedule (Table 8) Those previously vaccinated as shown in the table above will receive vaccines at the times specified in the first item according to the procedure described below. 2.B. Schedule (Table 9) (39): 3. Vaccinations will be administered to all officers and enlisted personnel without exception. 4. It is recommended that vaccinations be administered without delay, as a delayed response may result in a delayed immune response. 5. Vaccinations will be recorded in the soldiers’ identity records on a daily basis. 6. Enlisted personnel who are to be deployed on duty, on leave, or due to a change of station, or who are discharged from hospitals, must have been vaccinated against cholera no more than two months prior and against typhus no more than four months prior to their departure. Those vaccinated within these periods will be revaccinated, and the vaccination dates will be recorded in their documents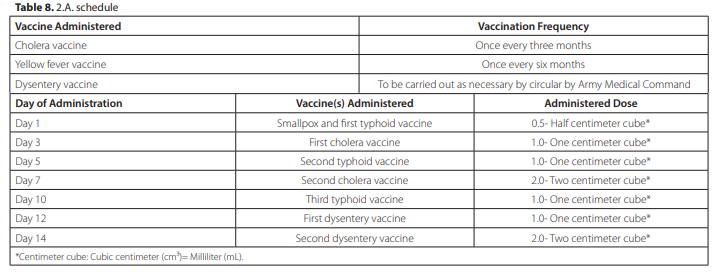

.7. It is the duty of commanders to ensure that no one remains unvaccinated before the movement of units. 8. Supply soldiers will be vaccinated primarily at assembly or cleaning locations, according to Schedule 2.A. (Table 8). 9. Units dispatched to epidemic areas, as well as officers and soldiers sent individually, must be revaccinated according to Schedule 2.B. (Table 9) based on the type of epidemic. This directive clearly demonstrates how vaccination practices were carried out in a planned and centralized manner within the Ottoman military health system. It is evident that procedures were meticulously regulated regarding the repetition of vaccinations at specific intervals according to vaccine type, the implementation of a phased vaccination schedule for new recruits, and the re-vaccination of previously vaccinated personnel. The mandatory nature of vaccination, regardless of rank, and the recording of all procedures indicate that vaccination activities were considered a fundamental preventive health measure in the prevention of epidemic diseases. In this respect, the directive clearly documents that health services on the Gallipoli Front were approached within the framework of a preventive medicine approach based on vaccination rather than curative interventions. Thanks to the quarantine stations, significant benefits were achieved at the Gallipoli Front; the spread of major epidemic diseases and the potential loss of life they could cause were prevented. In addition to soldiers, vaccination was also administered to doctors, nurses, and orderlies providing primary care to wounded soldiers. At the same time, vaccination programs were implemented as much as possible under the conditions of the time to protect the public from infectious diseases (29). Limited opportunities for personal hygiene and changing clothes in trench conditions led to lice infestations, resulting in an increase in typhus cases. Of the 149 soldiers who contracted typhus, 36 lost their lives (40). Despite all of these adverse conditions, Mr. Cemil (Conk), Commander of the 4th Division, explains in his memoirs the reason why the mortality rate remained relatively low. According to Mr. Cemil (Conk), the vaccination of soldiers with cholera and typhus vaccines delivered to the front on August 25, 1915, played a decisive role in keeping deaths to a minimum during this period (41,42). In the search for a solution to typhus, Ottoman physician Mr. Reşat Rıza (Kor), together with his colleague Mr. Mustafa Hilmi (Sağun), developed a vaccine in 1914 based on inactivating the agent (Rickettsia prowazekii) found in the blood of typhus patients, even though the cause of the disease had not yet been clearly identified by the scientific community (43-46). As they described, the production procedure for this vaccine was as follows: “10-20 cubic centimeters of blood taken from a typhus patient with a high fever in the advanced stages of the disease is placed in a sterile bottle containing sterile glass beads. After the blood is thoroughly shaken, the fibrin is completely separated. The bottle containing the blood separated from the fibrin should then be kept in 60°C water for one hour, shaking it frequently. In this way, the typhus agent in the blood is rendered harmless, and the material obtained can be used as a typhus vaccine. It is sufficient to inject 5 cubic centimeters of this preparation under the skin of the soldier to whom the vaccine will be administered” (45). In addition, Dr. Abdülkadir Lütfi (Noyan), one of the Ottoman military doctors, administered the typhus vaccine to 76 officers, 30 doctors, and 20 nurses within the 6th Army in Baghdad. Noyan states that the vaccine in question was also administered at the Kut al-Amara Front. In contrast, the commander of the 6th Army, Colmar Freiherr von der Goltz Pasha, refused to be vaccinated due to the objection of his personal physician; later, both he and his physician died of typhus (47). Abdülkadir Lütfi (Noyan) stated that only one person died in relation to the typhus vaccination, and that this was due to suicide: “I vaccinated 30 doctors, 76 officers, and 20 nurses with the vaccine I administered at the army headquarters. During the entire war, three of these doctors contracted the disease, and one committed suicide. There were no other deaths. None of the officers contracted typhus. Two of the 20 nurses fell ill 3-4 days after vaccination. Their illness was relatively mild; one fell ill 30 days later and recovered very quickly” (48). Within the framework of vaccination activities, Bacteriologist Dr. Tevfik İsmail was assigned by Second Army Health Inspector Dr. Tevfik Salim to implement the dysentery vaccine introduced in Çanakkale and to examine the level of immunity on the Anatolian side (36). Again on this matter, an order signed by Liman von Sanders, who was responsible for the Çanakkale Front, defined the areas of responsibility of the laboratories in İzmir, Aydın, and Bandırma and requested that bacteriological studies be carried out within these areas. The same order specifically emphasized that it was also necessary to prepare the vaccines needed by the army (49). Vaccination Center and Vaccine Supply to the Front During wars, vaccines were among the most needed medical supplies. In order to ensure the production of smallpox vaccines, the first vaccination center was established in İstanbul; following this initiative, vaccination centers were established throughout the country. The main reason for this was that vaccines sent to provinces far from İstanbul were spoiled during the long journey when the disease appeared in those regions. In addition, the emergence of smallpox in places far from the center made it very difficult to supply vaccines. This situation led to the intensification of smallpox and, consequently, an increase in deaths. For this reason, work began on opening a vaccination center in the province of Yemen, which was very far from the center, i.e., İstanbul (50-52). Furthermore, due to their distance from the center, it was decided to establish vaccination centers in places such as Haydarpaşa, Syria, Mosul, and Erzurum. The operation of these vaccination centers made it possible to produce smallpox vaccine in a short time and to carry out a rapid vaccination process throughout the country when needed. This provided an effective intervention to control the spread of the disease and reduce mortality rates (53,54). It is understood that during the battles, 15 kilograms of cholera vaccine, 20.000 doses of smallpox vaccine, and 60 doses of tetanus vaccine were requested from the Field Medical Department and delivered to the front (55,56). Furthermore, on May 19, 1915, the 5th Army Command requested that the Field Medical Department send 6.000 smallpox vaccines and 15 kilograms of cholera vaccine to Akbaş, in line with the needs of the hospitals. On May 26, 1915, 2.000 doses of cholera, typhoid, and smallpox vaccines were sent; on May 28, 1915, sufficient quantities of smallpox, cholera, and typhoid vaccines were sent to Bandırma for the chief medical officers of the 7th and 8th Divisions; On June 13, 1915, 100 kilograms of cholera vaccine and as much typhoid and smallpox vaccine as possible were requested. On August 23, 1915, due to the arrival of new soldiers every day, the number of soldiers at the 12th Depot Battalion in Tekirdağ reached 3.000, and therefore, the 3rd Corps Command requested typhoid and cholera vaccines to be delivered before the dispatch. The 3rd Corps Command’s vaccine requests continued throughout the battles (55,56). On October 1, 1915, vaccines were requested for soldiers ready for deployment in Bandırma, Bursa, and Tekirdağ. Accordingly, on October 7, 1915, 10 kilograms of dysentery vaccine were sent to Tekirdağ on behalf of the 3rd Corps. On October 27, 1915, 30 kilograms of dysentery vaccine, 17 kilograms of cholera vaccine, 20 kilograms of typhoid vaccine, and 20 doses of dysentery serum were sent to the Menzil Medical Depot in Lapseki (55). If necessary, vaccinations continued at the front. The order regarding this was “Fresh dysentery and cholera vaccines will be administered.” This situation is also reflected in the memoirs of many officers. In his memoirs, Mr. Cemil (Conk), Commander of the 4th Division, wrote on August 25, 1915, “Today, cholera and typhoid vaccines arrived. We vaccinated the soldiers“; İzzettin Çalışlar, on July 31, 1915, wrote “I was vaccinated with the typhoid vaccine. The vaccine had a very strong effect“; Mr. Fasih, on November 18, 1915, wrote “The troops are being vaccinated against dysentery” (29,56).